
2022.12.30
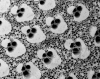
CharXgen活性竹炭包裹在海藻酸鈉微球中作為尿毒症毒素的吸收劑以延緩腎功能惡化新知導讀-CharXgen活性竹炭包裹在海藻酸鈉微球中作為尿毒症毒素的吸收劑以延緩腎功能惡化 by: agnes30 12 月, 2022 本篇文章導讀自: CharXgen-Activated Bamboo Charcoal Encapsulated in Sodium Alginate Microsphere as the Absorbent of Uremic Toxins to Retard Kidney Function Deterioration 以新型活性碳CharXgen餵食CKD大鼠,發現具有保護腎功能及降低血清尿毒症的潛在益處 | 摘要 硫酸吲哚酚 (IS) 和對甲酚硫酸鹽 (PCS) 是慢性腎病 (CKD) 中積累的兩種蛋白質結合尿毒症毒素。本研究的目的是評估新型活性炭 CharXgen 在 CKD 動物模型中對保護腎功能和降低血清尿毒症毒素的影響。 透過掃描電子顯微鏡 (SEM) 和 X 射線衍射儀 (XRD) 對活化前後的CharXgen進行物理特性分析,發現活化後的CharXgen 比表面積增加。 透過體外結合試驗和 CKD 動物模型評估 CharXgen 對生物化學和降低尿毒症毒素的影響。動物試驗總共分成五組,分別是正常組、假手術組(對動物進行和實驗組相同的手術處理,但並不給予實驗刺激)、CKD組、CKD + AST-120組與CKD+CharXgen組。 經掃描電子顯微鏡 (SEM) 和 X 射線衍射儀 (XRD) 分析後發現活化後的CharXgen 具有高內表面積。經體外結核試驗發現CharXgen 能夠有效吸收硫酸吲哚酚及對甲酚硫酸鹽。而在動物實驗中,CKD+CharXgen組的大鼠腎功能獲得改善,且血清中 IS 和 PCS 較低。另外,與 CKD 組相比,發現CKD+CharXgen組的大鼠成纖維細胞生長因子 23 顯著降低,這種變化在CKD + AST-120組未發現。這表明 CharXgen 是一種新型安全無毒的活性炭,具有減輕腎功能惡化和降低與蛋白質結合的尿毒症毒素的潛力。 l 簡介 患有慢性腎病 (CKD) 的患者患心血管疾病 (CVD) 的風險顯著增加,尤其是患有終末期腎病 (ESRD) 的患者。傳統的CVD高風險族群如高血壓、高血脂症和糖尿病患者不能完全解釋CVD增加的風險;而CKD患者這種非傳統的風險因子則有明確的證據支持,其中包括尿毒症毒素的積累、腎功能下降及尿毒症溶質。 尿毒症溶質包括硫酸吲哚酚 (IS) 和對甲酚硫酸鹽 (PCS),它們是腸道菌群代謝芳香氨基酸後源自腸道的兩種蛋白質結合尿毒症毒素,會抑制內皮細胞增殖,可能導致內皮細胞功能的障礙 。而IS 的積累可能會加速腎小球硬化、氧化應激、間質纖維化及腎元減少而促進CKD的進展。IS 參與了 CKD 中 CVD 的發病機制,包括動脈粥樣硬化、外周動脈疾病、充血性心力衰竭、血栓形成和心律失常。另外,成纖維細胞生長因子 23 (FGF23) 是一種從骨分泌的磷酸尿因子,在腎臟功能衰退初期,血中FGF23的濃度即升高。FGF 23 不僅是礦物質骨紊亂的主要調節因子,而且還是導致 CKD 患者心血管發病率和死亡率的因素。因此,減少體內IS 和 PCS的濃度及降低FGF23可能可以延緩CKD的進展。 AST-120 是1991年在日本上市的口服腸道吸附劑,可透過減少 CKD 患者的炎症基因表現,有效降低血清和尿液的 IS 濃度並延緩 CKD 進展的藥物 。在美國的一項初步隨機、雙盲、安慰劑對照試驗中,AST-120 與血清 IS水平的顯著劑量依賴性降低和尿毒症相關不適的減少有關。 因此,通過 AST-120 去除 IS 不僅改善了腎功能,還降低了 CKD 患者心血管事件的風險。 但是AST-120的生產成本較高,所以應用並不廣泛。不過,還有一種從台灣竹子萃取及生產的新型活性炭 CharXgen,具有多孔結構,其安全性、腎臟保護作用以及是否可以降低血清生化指標尚不清楚。因此,作者的目的是研究 CharXgen 對 CKD 動物模型臨床參數的影響。 l 結果 圖 1.掃描電子顯微鏡 (SEM) 分析的竹炭 ( A , B ) 和 CharXgen ( C , D ) 的橫截面和縱截面。 發現Brunauer-Emmett-Teller (BET)比表面積值在竹炭活化過後顯著增加。 圖 2.比較CharXgen及AST-120 在胃腸模擬狀態下吲哚 ( A )、對甲酚 ( B ) 和磷酸鹽 ( C ) 的體外結合能力測定。 在小腸和大腸等條件下,CharXgen 對吲哚的結合親和力更高(圖 2A) 在小腸條件下,CharXgen與對甲酚的結合親和力更高;在大腸條件下,CharXgen 和 AST-120 之間的對甲酚結合親和力沒有顯著差異(圖 2B) 在口腔條件下,CharXgen對磷酸鹽的結合能力與 AST-120 相似;在胃、小腸和大腸條件下,AST-120對磷酸鹽結合能力更高,(圖 2C) 圖 3. 每組大鼠分別在餵食木炭、AST-120 或 CharXgen 後 8、16 和 24 小時的腸道狀態。 結果顯示CharXgen組腸道顏色結果與AST-120組相似,與木炭組相比沒有明顯變黑。 圖 4. 每組大鼠的肝功能和營養狀況。各組GPT( A)和GOT(B)及白蛋白(C)水平無顯著差異。 GPT:谷丙轉氨酶;GOT:谷氨酸草酰乙酸轉氨酶。 CKD + AST-120組 和 CKD + CharXgen 組的肝功能,與正常組或假手術組相比沒有顯著變化(圖 4 A,B) 在血清白蛋白方面,CKD組和CKD+CharXgen組也呈現正常水平(圖4 C) 圖 5. 每組大鼠的腎功能。BUN:血尿素氮;Cr:肌酐 與 CKD 組相比,CKD + CharXgen 組的血清 BUN ( A ) 和 Cr ( B ) 水平顯著降低。 圖 6.每組大鼠的血清鈣 ( A )、磷酸鹽 ( B ) 和 FGF23 ( C ) 水平。(FGF23:成纖維細胞生長因子 23) 每組的鈣和磷酸鹽沒有顯著變化。而在FGF23中顯示CKD + CharXgen 組大鼠的 FGF23 與 CKD 組相比,水平較低。 | 結論 結果顯示 CharXgen新型活性碳具有很大的比表面積及多孔特性,且在體內安全無毒。此外,透過上述實驗發現 CharXgen 在保護大鼠腎功能和降低尿毒症有潛在益處,可能可以減輕 CKD 大鼠腎功能惡化和降低 IS 和、PCS及 FGF23 水平的潛力。不過CharXgen是否在人體腎臟中的具有保護作用還需要再進一步的研究。 l 參考文獻 Vanholder, R.; Massy, Z.; Argiles, A.; Spasovski, G.; Verbeke, F.; Lameire, N.; European Uremic Toxin Work Group. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol. Dial. Transplant 2005, 20, 1048–1056. [Google Scholar] [CrossRef][Green Version] Levin, A.; Foley, R.N. Cardiovascular disease in chronic renal insufficiency. Am. J. Kidney Dis. 2000, 36, S24–S30. [Google Scholar] [CrossRef] Weiner, D.E.; Tighiouart, H.; Amin, M.G.; Stark, P.C.; MacLeod, B.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: A pooled analysis of community-based studies. J. Am. Soc. Nephrol. 2004, 15, 1307–1315. [Google Scholar] [CrossRef] Weiner, D.E.; Tighiouart, H.; Elsayed, E.F.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. The relationship between nontraditional risk factors and outcomes in individuals with stage 3 to 4 CKD. Am. J. Kidney Dis. 2008, 51, 212–223. [Google Scholar] [CrossRef][Green Version] Longenecker, J.C.; Coresh, J.; Powe, N.R.; Levey, A.S.; Fink, N.E.; Martin, A.; Klag, M.J. Traditional cardiovascular disease risk factors in dialysis patients compared with the general population: The CHOICE Study. J. Am. Soc. Nephrol. 2002, 13, 1918–1927. [Google Scholar] [CrossRef][Green Version] Clarke, R.; Daly, L.; Robinson, K.; Naughten, E.; Cahalane, S.; Fowler, B.; Graham, I. Hyperhomocysteinemia: An independent risk factor for vascular disease. N. Engl. J. Med. 1991, 324, 1149–1155. [Google Scholar] [CrossRef] Appel, L.J. Beyond (or Back to) Traditional Risk Factors: Preventing Cardiovascular Disease in Patients with Chronic Kidney Disease. Ann. Intern. Med. 2004, 140, 60–61. [Google Scholar] Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 2003, 42, 1050–1065. [Google Scholar] [CrossRef] Lin, C.J.; Wu, C.J.; Pan, C.F.; Chen, Y.C.; Sun, F.J.; Chen, H.H. Serum protein-bound uraemic toxins and clinical outcomes in haemodialysis patients. Nephrol. Dial. Transplant. 2010, 25, 3693–3700. [Google Scholar] [CrossRef][Green Version] Dou, L.; Bertrand, E.; Cerini, C.; Faure, V.; Sampol, J.; Vanholder, R.; Berland, Y.; Brunet, P. The uremic solutes p-cresol and indoxyl sulfate inhibit endothelial proliferation and wound repair. Kidney Int. 2004, 65, 442–451. [Google Scholar] [CrossRef] Tumur, Z.; Niwa, T. Indoxyl Sulfate Inhibits Nitric Oxide Production and Cell Viability by Inducing Oxidative Stress in Vascular Endothelial Cells. Am. J. Nephrol. 2009, 29, 551–557. [Google Scholar] [CrossRef] Motojima, M.; Hosokawa, A.; Yamato, H.; Muraki, T.; Yoshioka, T. Uremic toxins of organic anions up-regulate PAI-1 expression by induction of NF-κB and free radical in proximal tubular cells. Kidney Int. 2003, 63, 1671–1680. [Google Scholar] [CrossRef][Green Version] Gelasco, A.K.; Raymond, J.R. Indoxyl sulfate induces complex redox alterations in mesangial cells. Am. J. Physiol. Renal Physiol. 2006, 290, F1551–F1558. [Google Scholar] [CrossRef][Green Version] Ito, S.; Osaka, M.; Higuchi, Y.; Nishijima, F.; Ishii, H.; Yoshida, M. Indoxyl sulfate induces leukocyte-endothelial interactions through up-regulation of E-selectin. J. Biol Chem. 2010, 285, 38869–38875. [Google Scholar] [CrossRef][Green Version] Dou, L.; Burtey, S. The harmful effect of indoxyl sulfate on neovascularization in chronic kidney disease. Kidney Int. 2016, 89, 532–534. [Google Scholar] [CrossRef][Green Version] Lekawanvijit, S.; Kompa, A.R.; Manabe, M.; Wang, B.H.; Langham, R.G.; Nishijima, F.; Kelly, D.J.; Krum, H. Chronic kidney disease-induced cardiac fibrosis is ameliorated by reducing circulating levels of a non-dialysable uremic toxin, indoxyl sulfate. PLoS ONE. 2012, 7, e41281. [Google Scholar] [CrossRef][Green Version] Chitalia, V.C.; Shivanna, S.; Martorell, J.; Balcells, M.; Bosch, I.; Kolandaivelu, K.; Edelman, E.R. Uremic serum and solutes increase post-vascular interventional thrombotic risk through altered stability of smooth muscle cell tissue factor. Circulation 2013, 127, 365–376. [Google Scholar] [CrossRef] Hung, S.C.; Kuo, K.L.; Huang, H.L.; Lin, C.C.; Tsai, T.H.; Wang, C.H.; Chen, J.W.; Lin, S.J.; Huang, P.H.; Tarng, D.C. Indoxyl sulfate suppresses endothelial progenitor cell–mediated neovascularization. Kidney Int. 2016, 89, 574–585. [Google Scholar] [CrossRef][Green Version] Bammens, B.; Evenepoel, P.; Keuleers, H.; Verbeke, K.; Vanrenterghem, Y. Free serum concentrations of the protein-bound retention solute p-cresol predict mortality in hemodialysis patients. Kidney Int. 2006, 69, 1081–1087. [Google Scholar] [CrossRef] Meijers, B.K.; Bammens, B.; De Moor, B.; Verbeke, K.; Vanrenterghem, Y.; Evenepoel, P. Free p-cresol is associated with cardiovascular disease in hemodialysis patients. Kidney Int. 2008, 73, 1174–1180. [Google Scholar] [CrossRef][Green Version] Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A.; European Uremic Toxin Work Group (EUTox). Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef] [PubMed][Green Version] Lin, C.J.; Wu, V.; Wu, P.C.; Wu, C.J. Meta-Analysis of the Associations of p-Cresyl Sulfate (PCS) and Indoxyl Sulfate (IS) with Cardiovascular Events and All-Cause Mortality in Patients with Chronic Renal Failure. PLoS ONE 2015, 10, e0132589. [Google Scholar] [CrossRef] [PubMed] Gutierrez, O.; Isakova, T.; Rhee, E.; Shah, A.; Holmes, J.; Collerone, G.; Jüppner, H.; Wolf, M. Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J. Am. Soc. Nephrol. 2005, 16, 2205–2215. [Google Scholar] [CrossRef] [PubMed] Lin, C.J.; Pan, C.F.; Chuang, C.K.; Liu, H.L.; Sun, F.J.; Wang, T.J.; Chen, H.H.; Wu, C.J. Association of Indoxyl Sulfate with Fibroblast Growth Factor 23 in Patients with Advanced Chronic Kidney Disease. Am. J. Med. Sci. 2014, 347, 370–376. [Google Scholar] [CrossRef] Isakova, T.; Xie, H.; Yang, W.; Xie, D.; Anderson, A.H.; Scialla, J.; Wahl, P.; Gutiérrez, O.M.; Steigerwalt, S.; He, J.; et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 2011, 305, 2432–2439. [Google Scholar] [CrossRef][Green Version] Nakano, C.; Hamano, T.; Fujii, N.; Obi, Y.; Matsui, I.; Tomida, K.; Mikami, S.; Inoue, K.; Shimomura, A.; Nagasawa, Y.; et al. Intactfibroblast growth factor 23 levels predict incident cardiovascular event before but not after the start of dialysis. Bone 2012, 50, 1266–1274. [Google Scholar] [CrossRef] Schulman, G.; Agarwal, R.; Acharya, M.; Berl, T.; Blumenthal, S.; Kopyt, N. A multicenter, randomized, double-blind, placebo-controlled, dose-ranging study of AST-120 (Kremezin) in patients with moderate to severe CKD. Am. J. Kidney Dis. 2006, 47, 565–577. [Google Scholar] [CrossRef] Goto, S.; Kitamura, K.; Kono, K.; Nakai, K.; Fujii, H.; Nishi, S. Association between AST-120 and abdominal aortic calcification in predialysis patients with chronic kidney disease. Clin Exp. Nephrol. 2013, 17, 365–371. [Google Scholar] [CrossRef] Marier, J.F.; Lee, J.; Kambhampati, S.R.; Galitz, L.; Vargas, R.; Moberly, J.; Salazar, D.E. Effect of repeated oral administrations of the oral adsorbent AST-120 on serum creatinine and other markers of renal function. A randomized controlled study in patients with chronic kidney disease. Am. J. Nephrol. 2006, 26, 136–141. [Google Scholar] [CrossRef] Akizawa, T.; Asano, Y.; Morita, S.; Wakita, T.; Onishi, Y.; Fukuhara, S.; Gejyo, F.; Matsuo, S.; Yorioka, N.; Kurokawa, K.; et al. CAP-KD Study Group, Effect of a carbonaceous oral adsorbent on the progression of CKD: A multicenter, randomized, controlled trial. Am. J. Kidney Dis. 2009, 54, 459–467. [Google Scholar] [CrossRef] Fujii, H.; Nishijima, F.; Goto, S.; Sugano, M.; Yamato, H.; Kitazawa, R.; Kitazawa, S.; Fukagawa, M. Oral charcoal adsorbent (AST-120) prevents progression of cardiac damage in chronic kidney disease through suppression of oxidative stress. Nephrol. Dial. Transplant. 2009, 24, 2089–2095. [Google Scholar] [CrossRef][Green Version] Nakai, K.; Fujii, H.; Kono, K.; Goto, S.; Fukagawa, M.; Nishi, S. Effects ofAST-120on left ventricular mass in predialysis patients. Am. J. Nephrol. 2011, 33, 218–223. [Google Scholar] [CrossRef] Vanholder, R.; Smet, R.D. Pathophysiologic effects of uremic retention solutes. J. Am. Soc. Nephrol. 1999, 10, 1815–1823. [Google Scholar] Lin, C.J.; Liou, T.C.; Pan, C.F.; Wu, P.C.; Sun, F.J.; Liu, H.L.; Chen, H.H.; Wu, C.J. The Role of Liver in Determining Serum Colon-Derived Uremic Solutes. PLoS ONE 2015, 10, e0134590. [Google Scholar] [CrossRef] Aronov, P.A.; Luo, F.J.; Plummer, N.S.; Quan, Z.; Holmes, S.; Hostetter, T.H.; Meyer, T.W. Coloniccontribution to uremicsolutes. J. Am. Soc. Nephrol. 2011, 22, 1769–1776. [Google Scholar] [CrossRef][Green Version] Atkinson, S.W.; Young, Y.; Trotter, G.A. Treatment with activated charcoal complicated by gastrointestinal obstruction requiring surgery. BMJ 1992, 305, 563. [Google Scholar] [CrossRef][Green Version] Moe, S.; Drüeke, T.; Cunningham, J.; Goodman, W.; Martin, K.; Olgaard, K.; Ott, S.; Sprague, S.; Lameire, N.; Eknoyan, G.; et al. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006, 69, 1945–1953. [Google Scholar] [CrossRef][Green Version] Parker, B.D.; Schurgers, L.J.; Brandenburg, V.M.; Christenson, R.H.; Vermeer, C.; Ketteler, M.; Shlipak, M.G.; Whooley, M.A.; Ix, J.H. The associations of fibroblast growth factor 23 and uncarboxylated matrix Gla protein with mortality in Coronary artery disease: The heart and soul study. Ann. Intern. Med. 2010, 152, 640–648. [Google Scholar] [CrossRef][Green Version] Gutiérrez, O.M.; Januzzi, J.L.; Isakova, T.; Laliberte, K.; Smith, K.; Collerone, G.; Sarwar, A.; Hoffmann, U.; Coglianese, E.; Christenson, R.; et al. Fibroblast growth factor 23 and left ventricular hypertrophy in chronic kidney disease. Circulation 2009, 119, 2545–2552. [Google Scholar] [CrossRef][Green Version] Fliser, D.; Kollerits, B.; Neyer, U.; Ankerst, D.P.; Lhotta, K.; Lingenhel, A.; Ritz, E.; Kronenberg, F.; MMKD Study Group; Kuen, E.; et al. Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: The Mild to Moderate Kidney Disease (MMKD) Study. J. Am. Soc. Nephrol. 2007, 18, 2600–2608. [Google Scholar] [CrossRef] Larsson, T.; Nisbeth, U.; Ljunggren, O.; Juppner, H.; Jonsson, K.B. Circulating concentration of FGF-23 increases as renal function declines in patients with chronic kidney disease, but does not change in response to variation in phosphate intake in healthy volunteers. Kidney Int. 2003, 64, 2272–2279. [Google Scholar] [CrossRef][Green Version] Rodelo-Haad, C.; Rodríguez-Ortiz, M.E.; Martin-Malo, A.; Pendon-Ruiz de Mier, M.V.; Agüera, M.L.; Muñoz-Castañeda, J.R.; Soriano, S.; Caravaca, F.; Alvarez-Lara, M.A.; Felsenfeld, A.; et al. Phosphate control in reducing FGF23 levels in hemodialysis patients. PLoS ONE. 2018, 13, e0201537. [Google Scholar] [CrossRef] Francis, C.; David, V. Inflammation regulates fibroblast growth factor 23 production. Curr. Opin. Nephrol. Hypertens. 2016, 25, 325–332. [Google Scholar] [CrossRef][Green Version] Czaya, B.; Faul, C. TheRoleofFibroblast Growth Factor 23 in inflammation and Anemia. Int. J. Mol. Sci. 2019, 20, 4195. [Google Scholar] [CrossRef][Green Version] 文章出處:保健資訊總匯https://drippingpill.com.tw/

2022.06.27
醫學界正在研究 EPA 攝入量對 SARS感染患者的影響介紹 Omega-3 脂肪酸 (尤其是EPA) 能夠抑制促炎細胞因子的產生並產生更多的特殊解炎脂質介質 (SPM) (包括前列腺素、血栓素、保護素和分解素)。 在新冠病毒SARS-CoV-2 感染中,omega-3 脂肪酸可藉由調節脂質筏流動性來破S蛋白-ACE2 複合物的形成而發揮抑制新冠病毒進入細胞的作用。 目前,醫學界正在進行一項臨床試驗,研究 EPA 攝入量對 SARS-CoV-2 感染患者的影響。 本文章導讀自: Can N-3 polyunsaturated fatty acids be considered a potential adjuvant therapy for COVID-19-associated cardiovascular complications? 文章來源:https://pubmed.ncbi.nlm.nih.gov/33031856/
2022.06.01
活性碳膠囊與細粒、顆粒差異毒素在小腸末端(ileum)就開始產生及吸收了,還有些吃入的重金屬在胃腸就開始吸收,毒素一般 根本到不了大腸。 細粒附劑顆粒在胃腸是有選擇性的吸附,可以在胃腸就開始吸收毒素,作用比一般膠囊裝活性炭粉在大腸作用更完全。

2022.05.30
益生菌改善慢性便秘患者的糞便稠度新知導讀-益生菌改善慢性便秘患者的糞便稠度:一項隨機、雙盲、安慰劑對照研究 攝取植物乳桿菌(1億,持續4周)有助於改善慢性便秘患者的大便軟硬度,停止攝取後且可持續效果 本文章導讀自: Probiotics Ameliorate Stool Consistency in Patients with Chronic Constipation: A Randomized, Double-Blind, Placebo-Controlled Study 摘要 背景/目的: 在腸易激綜合徵便秘 (IBS-C) 或功能性便秘 (FC) 患者中研究益生菌在改善臨床症狀、改變糞便微生物群和調節血清免疫細胞因子水平方面的功效。 方法: 2016 年 10 月至 2017 年 2 月在韓國慶熙大學醫院進行了一項隨機、雙盲、安慰劑對照試驗。針對18-75 歲診斷為 IBS-C 或 FC 的患者(根據羅馬四準則),每天服用益生菌(3.0 × 10 8 CFU/g 嗜熱鏈球菌 MG510 和 1.0 × 10 8 CFU/g 植物乳桿菌 LRCC5193)或安慰劑,持續 4 週(第 1-4 週),隨後進行 4 週的清除期無需干預(第 5-8 週)。該研究的主要結果是根據布里斯託大便形式量表和完全自主排便(CSBM)評估功效。 結果: 通過布里斯託大便形式量表測量的大便稠度在益生菌組 (n = 88) 中明顯優於安慰劑組 (n = 83)(第 8 週時為 3.7 ± 1.1 vs. 3.1 ± 1.1 , P = 0.002),不過在CSBM中沒有發現顯著差異,另外,益生菌組的生活質量明顯好於安慰劑組。在 4 週時,益生菌組的糞便微生物組中植物乳桿菌的相對豐度顯著高於安慰劑組(P = 0.029)。然而,其他微生物組和血清細胞因子的水平(IL-10/IL-12 比率和 TNF-α)在兩組之間沒有顯著差異。 結論:益生菌可顯著改善慢性便秘患者的大便稠度。此外,在停止補充益生菌後,植物乳桿菌對糞便稠度的有益作用仍然存在。 簡介 便祕在一般人身上所發生的機率為5-20%,為最常見的消化系統疾病。其特徵為大便為塊狀或硬塊、排便次數較少、排便有不完全感等等[1, 2]。涉及便祕的兩種主要功能性腸病為腸易激綜合徵便秘 (IBS-C) 或功能性便秘 (FC) ,這兩種類性的腸病主要以有無腹痛來區分: IBS-C有明顯的腹痛、腹脹;FC則是缺乏器質性病因,沒有結構異常或代謝障礙,所以沒有明顯得腹痛[3, 4]。目前已被用於治療便秘的方法有很多,如膨化劑、灌腸劑、滲透性或刺激性瀉藥、飲食改變及行為改變,不過大約一半的患者對症狀不滿意[5]。 益生菌為宿主提供有益微生物群,可以改善便秘所引起的腸道微生物群紊亂[6, 7]。先前雖有研究益生菌對於IBS-C的治療作用,但結果不一致,有些研究效果有改善,有些研究則認為沒有明顯效果。 然而,2016所更新的 羅馬四準則 表明IBS-C和FC是連續存在的,而不是獨立的疾病,因为FC患者並沒有完全擺脫腹痛或腹脹[3,30]。 因此,在此研究旨在根據 羅馬四準則 將 IBS-C和FC納入慢性便秘,並探討益生菌在改善臨床症狀、改變糞便菌群及調節血清免疫細胞因子水平等方面的作用在慢性便秘(IBS-C或FC)病人身上的效果。 結果 在治療4周後,益生菌组的乳桿菌屬(Lactobacillus spp.)和植物乳桿菌(Lactobacillus plantarum)的相對豐富度顯著高於安慰組(P=0.049和P=0.029)。然而,乳桿菌屬的相對豐富度在8周之後下降到基限水平,而益生菌组的植物乳桿菌相對豐富度在8周時仍高於安慰劑組,但差異無統計學意義(2.19±0.77 vs. 1.00±0.16,P=0.137)。 另一組的嗜熱鏈球菌(Streptococcus thermoophilus)、雙歧桿菌(Bifdobacterium spp.)、擬桿菌門(Bacteroidetes spp.)和厚壁菌门(Firmicutes)的相對豐富度在研究期間均無明顯變化。(圖一) 結論 作者發現透過攝入益生菌,在4周改善慢性便秘患者的糞便一致性及糞便成分的微生物群,並且持續8周,尤其是 植物乳桿菌。同時,益生菌的攝入也改善了患者的生活質量。 參考文獻 1.Singh G, Lingala V, Wang H, et al. Use of health care resources and cost of care for adults with constipation. Clin Gastroenterol Hepatol. 2007;5:1053–1058. 2.Ford AC, Quigley EM, Lacy BE, et al. Efcacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: systematic review and meta-analysis. Am J Gastroenterol. 2014;109:1547–1561. 3.Mearin F, Lacy BE, Chang Let al. Bowel disorders. Gastroenterology. Epub. 02/18/2016. 4.Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology.2006;130:1480–1491. 5.Johanson JF, Kralstein J. Chronic constipation: a survey of the patient perspective. Aliment Pharmacol Ther. 2007;25:599–608. 6.Kassinen A, Krogius-Kurikka L, Makivuokko H, et al. The fecal microbiota of irritable bowel syndrome patients difers signifcantly from that of healthy subjects. Gastroenterology. 2007;133:24–33. 7.Attaluri A, Jackson M, Valestin J, Rao SS. Methanogenic fora is associated with altered colonic transit but not stool characteristics in constipation without IBS. Am J Gastroenterol. 2010;105:1407–1411.

2022.05.20
新知導讀-高濃度EPA改善ADHD過動兒及內源性 EPA低水平青少年的注意力及警惕性本篇文章導讀自: High dose eicosapentaenoic acid (EPA) improves attention and vigilance in children and adolescents with attention deficit hyperactivity disorder (ADHD) and low endogenous EPA levels l 摘要 作者進行了一項為期 12 週的雙盲安慰劑對照試驗,比較了高濃度二十碳五烯酸(EPA,1.2 g)和安慰劑對92名患有注意力缺陷多動障礙 (ADHD) 的6-18 歲青年。在治療前後測量血紅細胞的多元不飽和脂肪酸(PUFA) ,以檢查基線內源前後 EPA 水平對治療反應的影響以及 EPA 治療對 PUFA 水平的影響。次要指標包括其他 ADHD 症狀、情緒症狀以及血漿高敏 c 反應蛋白 (hs-CRP) 和腦源性神經營養因子 (BDNF) 的水平。在最後的實驗結果顯示,EPA 組在集中注意力方面比安慰劑組改善更多;另外,在基線內源性 EPA 水平最低的青少年中,EPA 組在集中注意力及警惕性的測量中也比安慰劑組改善更多。不過作者發現了一項有趣的現象,在具有最高基線 EPA 水平的青少年中,EPA 組在衝動性方面及情緒症狀方面的改善反而小於安慰劑組。EPA 使血液紅細胞 EPA 增加 1.6 倍,但不影響 DHA 、hs-CRP 和 BDNF 血漿水平。 總之,EPA 治療改善了 ADHD 青少年的認知症狀,倘若他們的基線內源性 EPA 水平較低改善程度會更加明顯,相反的, EPA 高水平的青少年可能會受到這種治療的負面影響。 l 簡介 N-3 多不飽和脂肪酸(N-3 PUFA)的主要成分為二十碳五烯酸 (EPA) 和二十二碳六烯酸 (DHA),是我們大腦和身體的必需脂肪酸 (EFA) 2,這些必需脂肪酸與認知功能3和學習成績4密切相關。近期的統合分析表明,與正常發育的青少年相比,患有 ADHD青少年的 DHA、EPA 和總 N-3 多不飽和脂肪酸的血液水平較低1。另外,在患有 ADHD 的兒童中發現EFA 缺乏症,而此症狀的嚴重程度被發現與 ADHD 症狀的嚴重程度有關6(EFA 缺乏症會出現過度口渴、皮膚乾燥、指甲變脆和小皮膚腫塊的症狀)。 ADHD一般來說會使用藥物治療,雖然這些治療具有良好的耐受性及治療效果,但同時也帶有些許副作用,需要長期追蹤觀察。而N-3 PUFA 具有非常好的耐受性和安全性,最近的統合分析顯示,使用n-3 PUFA 治療可改善ADHD青少年的臨床症狀,因此可能是患有多動症的青少年的治療首選。雖然個別研究有相互矛盾的發現,可能是因為不同研究中使用的 EPA 和 DHA 劑量不同所導致的。值得注意的是,之前對 ADHD 兒童臨床試驗進行的統合分析表明,需要高劑量的 omega-3(1-2 克)補充劑才能顯著改善臨床症狀11。儘管先前有證據表明EPA在抑鬱症的治療比DHA有效果 14 – 16 ,然而,針對 ADHD 與 n-3 PUFA之間的研究大多數使用高劑量 DHA 12或相對低劑量的 DHA 和 EPA 組合治療13。事實上,作者們的統合分析1表明,只有每天補充 ≥ 500毫克的EPA才能改善臨床過動衝動的症狀。 最後,就支持n-3 PUFA治療多動症的可能機制而言,有一些證據表明 ADHD 與炎症增加及神經水平降低有關: ADHD 兒童更容易患哮喘和特應性皮炎20 , 21,有兩項研究發現 ADHD 兒童的白細胞介素 IL-6 增加22 , 23 。 神經營養因子,如腦源性神經營養因子 (BDNF),也可能在 ADHD 中發揮作用24。 PUFA 通常被認為可調節神經可塑性25並具有抗炎作用26 ; 事實上,先前研究顯示,用 EPA 預處理可以減少由促炎細胞因子 IFN-α 16誘導的抑鬱症的發作。因此,這兩個生物系統可能與多不飽和脂肪酸在 ADHD 中的作用機制有關。 基於上述知識差距,我們在患有 ADHD 的青年(6-18 歲)中進行了一項為期 12 週的雙盲、隨機、安慰劑對照試驗 (RCT),其中比較了: (1) 高劑量的EPA(1.2 克/天)與安慰劑 (2) 測量認知功能作為主要結果 (3) 檢查內源性 PUFAs 水平以對患者進行分層並檢查治療對 PUFAs 水平的影響 (4) 研究炎症生物標誌物、高敏 CRP (hs-CRP) 和神經營養因子 BDNF 作為潛在機制 l 結果與結論 在 12 週結束時,有接受 EPA 的青少年顯示,血液紅細胞 EPA 和總 n-3 PUFA 水平增加,而 n-6/n-3 比率降低,這是一個預期的發現,它證實了年輕人對治療的依從性。主要結果測量是持續表現測試 (CPT) 的四個項目,分別測量集中注意力、衝動性、持續注意力和警惕性,在基線和第 12 週(試驗結束)進行評估。作者比較了 EPA 和安慰劑對 ADHD 的認知和臨床症狀以及機械相關生物標誌物的影響。發現EPA在改善集中注意力的項目中表現良好,這是我們的主要結果衡量指標之一。此外,內源性EPA 水平低的年輕人使用EPA後在進一步的注意力 (HRT) 和警覺性 (HRTISIC) 方面表現出更強的效果,兩者的改善都比安慰劑組要好。這是第一篇EPA 單一療法對 ADHD 影響的研究,也是有史以來第一篇使用內源性基線 PUFA 水平對 PUFA 臨床試驗中的受試者進行分層的研究。而進一步的研究顯示,對那些內源性EPA水平高的人進行EPA治療可能會產生不利影響。

2022.05.20
鼠李糖乳桿菌對減少兒童糞便輪狀病毒脫落量的劑量依賴性作用文章導讀自: Dose-dependent effect of Lactobacillus rhamnosus on quantitative reduction of faecal rotavirus shedding in children 摘要 背景/目的: 乳酸菌對兒童急性感染性腹瀉的有益作用主要為水樣腹瀉和病毒性胃腸炎,而鼠李糖乳桿菌是研究最廣泛的益生菌菌株之一,可有效縮短兒童急性腹瀉的病程。不過,鼠李糖乳桿菌在定量測定人類糞便輪狀病毒脫落時的劑量依賴效應尚不清楚。 方法:在23名患有急性輪狀病毒胃腸炎的兒童中進行了一項開放標籤隨機試驗。 患者被隨機分配成三種不同方案,並進行為期 3 天的試驗: 對照組: 6名患者接受每天 0 CFU的鼠李糖乳桿菌 低劑量組: 9 名患者每天 2 x 10 8 CFU的鼠李糖乳桿菌 高劑量組: 8 名患者每天 6 x 10 8 CFU的鼠李糖乳桿菌 在 3 天方案之前和之後收集糞便樣本,並透過 ELISA 測量輪狀病毒濃度。 結果: 無論是對照組(119.2 x 105 顆粒/ml vs. 23.7 x 105 顆粒/ml,p = 0.075)還是低劑量組(36.1 x 105 個顆粒/ml vs. 73.5 x 105 個顆粒/ml,p = 0.859),糞便輪狀病毒濃度的變化均無顯著變化,而高劑量組的糞便輪狀病毒濃度顯著降低(64.2 x 105顆粒/ml vs. 9.0 x 105 顆粒/ml,p = 0.012)。與給藥前相比,高劑量組內的 8 名患者的糞便輪狀病毒濃度在 3 天後均下降了 86%。 簡介 迄今為止,乳酸菌對兒童急性感染性腹瀉的有益程度似乎是中度,並且有菌株及劑量依賴性的作用。有文獻顯示如果在疾病早期就開始使用益生菌治療,效果會更加明顯[1]。鼠李糖乳桿菌在人體腸道中可以讓小兒輪狀病毒所引起的急性水樣腹瀉恢復得更快速[2]。 目前已有許多鼠李糖乳桿菌在不同模型中的劑量依賴效應紀錄: 鼠李糖乳桿菌對新生兔模型中的細菌易位有抑制作用[3] 鼠李糖乳桿菌在體外細胞培養模型中以劑量依賴的方式抑制大腸桿菌的易位[3] 鼠李糖乳桿菌在狗胃腸道存活能力和口服鼠李糖乳桿菌的安全性之評估,發現在為期五天的試驗中鼠李糖乳桿菌(5 x 10 11CFU)在糞便定殖的數量顯著增加[4] 連續3天以低、中、高劑量的鼠李糖乳桿菌在小牛早晨喝牛奶時一起餵食,發現餵食經過24小時後,鼠李糖乳桿菌的回收率分別為20%、80%和100%[5]。 益生菌已被證明對治療傳染性腹瀉以及减少腹瀉持續時間方面顯示出有益的效果,其中鼠李糖乳桿菌對輪狀病毒性腸胃炎的療效最顯著也最一致[1]。根據研究指出,乳酸菌每日劑量與腹瀉持續時間呈劑量依賴性反比關係,以>1011 CFU/48小時的劑量是最有效的[1]。然而,乳酸菌在其他應用中的劑量依賴效應,包括對糞便的影響、輪狀病毒在人體中的脫落,很少被拿來討論。因此作者設計了此隨機試驗來評估高劑量及低劑量的鼠李糖乳桿菌在定量減少兒童糞便輪狀病毒脫落方面是否存在潛在差異。 結果 糞便輪狀病毒濃度在服用安慰劑3天前後的比較發現對照組的病毒3天後表現出輕微的下降(方形和三角形表示每個病人糞便中輪狀病毒的濃度;水平線表示中位數) 糞便輪狀病毒濃度在服用高劑量鼠李糖乳桿菌3天後的比較發現高劑量組的病毒有顯著下降情形位(方形和三角形表示每個病人糞便中輪狀病毒的濃度;水平線表示中位數) 糞便輪狀病毒濃度在服用低劑量鼠李糖乳桿菌3天後的比較發現低劑量組的病毒濃度呈不同程度的升高或降低現象(方形和三角形表示每個病人糞便中輪狀病毒的濃度;水平線表示中位數) 結論 作者發現透過攝入不同劑量的鼠李糖乳桿菌,觀察糞便輪狀病毒的總數,高劑量組對比於低劑量組及對照組在食用後病毒總數有明顯下降的趨勢。 參考文獻 1.Szajewska H, Mrukowicz JZ. Use of probiotics in children with acute diarrhea. Paediatr Drugs.2005;7:111–22 2.Isolauri E, Kaila M, Mykkanen H, Ling WH Salminen S. Oral bacteriotherapy for viral gastroenteritis. Dig Dis Sci 1994;39:2595–600. 3.Mattar AF, Drongowski RA, Coran AG, Harmon CM.Effect of probiotics on enterocyte bacterial translocation in vitro. Pediatr Surg Int 2001;17:265–8. 4.Weese JS, Anderson ME. Preliminary evaluation of the probiotic potential of Lactobacillus rhamnosus strain GG, a potential probiotic in dogs. Can Vet J 2002;43:771–4. 5.Ewaschuk JB, Naylor JM, Chirino-Trejo M, Zello GA.Lactobacillus rhamnosus strain GG is a potential probiotic for calves. Can J Vet Res 2004;68:249–53.

2022.05.20
長雙歧桿菌 BB536 可緩解學齡前兒童的上呼吸道疾病並調節腸道微生物群文章導讀自: Bifidobacterium longum BB536 alleviated upper respiratory illnesses and modulated gut microbiota profiles in Malaysian pre-school children 摘要 背景/目的: 這項為期10個月的隨機雙盲、平行和安慰劑對照研究評估了長雙歧桿菌BB536對520名2-6歲健康學齡前兒童腹瀉和上呼吸道疾病的影響。 方法: 受試者每天隨機服用一克BB536 (5×109 cfu)或安慰劑,對219名完全依從超過10個月的受試者進行了數據分析(安慰劑n=110, BB536 n=109)。(其中301名沒有遵守醫囑導致數據缺失) 結果: 雖然BB536對兒童腹瀉無顯著影響,但數據顯示10個月以來平均呼吸道疾病次數組間存在顯著差異。咽喉痛持續時間減少46% (P=0.018),發燒持續時間略為減少27%(P=0.084)、流鼻涕减少15%(P=0.087)和咳嗽减少16%(P=0.087)。腸道菌群屬水平座標分析顯示,10月間的長雙歧桿菌對比0月在腸道菌群差異具有統計學意義。作者目前的研究說明了長雙歧桿菌對學齡前兒童上呼吸道疾病的潛在保護作用,及其對於腸道微生物群具有調節特性。 簡介 呼吸道疾病是兒童的主要健康問題之一,急性呼吸道感染是五歲以下兒童發病和死亡的主要元兇。上呼吸道感染(URTI)影響從鼻孔到喉部聲帶的氣道,表現症狀為普通感冒、中耳炎、咽炎、喉炎和鼻竇炎等症狀,是最常見的傳染疾病。在馬來西亞,急性呼吸道感染是季節性的,在年中(炎熱季節)和年底(雨季)流行率不斷增加。另外,急性腹瀉等胃腸疾病是全球五歲以下兒童發病及死亡的第二大原因。 人類胃腸道中密集分布500-1000種不同的細菌,其主要有4門,分別為厚壁菌門(Firmicutes)、擬桿菌門(Bacteroidetes)、變形菌門(Proteobacteria)和放線菌門(Actinobacteria)。有越来越多的證據表明,胃腸道微生物群落的失衡導致宿主免疫功能下降,增加罹患疾病的風險。 益生菌被定義為”適量使用可使宿主健康受益的活微生物”。在過去的二十年裡,益生菌因其從胃腸道健康到維生素合成和減輕代謝紊亂的益處而受到越来越多的關注。雙歧桿菌是與益生菌特性相關最常見的屬,並有充分的文獻證明可以增強免疫系统、緩解腹瀉,預防食物過敏和抗癌作用。 益生菌的目標和功效主要取决于菌株和宿主依賴因子,為臨床實驗中主要關注的議題之一,即透過精確的目標人群來確定和證明特定菌株對特定健康有益。作者目前的研究旨在透過10個月的隨機雙盲、平行和安慰劑對照研究,評估B. longum BB536對馬來西亞健康學齡前兒童腹瀉和上呼吸道疾病的影響。 結果 在10個月的研究期间,腹瀉臨床症狀總發生次數或天數的分組差異發現BB536組與安慰劑組對腹瀉天數、次數等胃腸道疾病均無顯著作用 在10個月的研究期間,BB536組和安慰劑组相比,喉嚨痛總天數少46.1% (P = 0.018),發燒持續時間降低27.8%(P = 0.084),流鼻涕降低13.2%(P = 0.087)和咳嗽降低16.3%(P = 0.087) 此圖為主坐標分析(PCoA)圖,比較了(A)安慰劑組和(B)長雙歧桿菌BB536組的在屬水平上對細菌分布的影響。 BB536組在0月到10月間出現顯著差異;安慰劑組則無出現顯著差異。 顯示攝入BB536對腸道菌群有調節作用 BB536組10個月後在普拉梭菌(Faecalibacterium)的豐富度與0個月相比出現顯著差異 結論 作者目前的研究表明口服 BB536 (每日5×109 cfu;每周5次),持續10個月,對2-6歲兒童的呼吸系统疾病有有益的效果。BB536在保護兒童免受呼吸系统疾病的發生次數、發燒、喉嚨痛、流鼻涕和咳嗽的持續時間方面更加普遍,而安慰劑沒有表現出這樣的好處。此外,BB536還調節了腸道微生物群,維持了普拉梭菌(Faecalibacterium)等有益微生物的豐富度,可以有效發揮其免疫調節作用。總之,作者目前的數據顯示,BB536是一種對兒童健康有益的益生菌,在上呼吸道疾病高發的季節具有潛在的保護作用。 參考文獻 1.Wang, Y., Li, X.L., Ge, T., Xiao, Y., Liao, Y., Cui, Y., Zhang, Y., Ho, W.,Yu, G. and Zhang, T., 2016. Probiotics for prevention and treatment of respiratory tract infections in children: a systematic review and meta-analysis of randomized controlled trials. Systematic Review and Meta-Analysis 95: 1-12. 2.Simoes, E.A.F., Cherian, T., Chow, J., Shahid-Salles, S.A., Laxminarayan, R. and John, T.J., 2006. Acute respiratory infections in children. In: Jamison, D.T., Breman, J.G., Measham, A.R., Alleyne, G., Claeson, M., Evans, D.B., Jha, P., Mills, A. and Musgrove, P. (eds.) Disease control priorities in developing countries. Oxford University Press, New York, NY, USA. 3.Lau, A.S.Y., Xiao, J.Z. and Liong, M.T., 2015. Bifidobacterium for infants: essence and efficacy. In: Liong, M.T. (ed.) Beneficial microorganisms in medical and health applications. Microbiology Monographs. Springer International Publishing, Cham, Switzerland, pp. 39-72. 4.Ewe, J.A., Wan-Abdullah, W.N. and Liong, M.T., 2010. Viability and growth characteristics of Lactobacillus in soymilk supplemented with B-vitamins. International Journal of Food Sciences and Nutrition 61: 87-107.

2022.05.20
副乾酪乳桿菌對皮膚反應性影響的隨機雙盲安慰劑對照研究文章導讀自: Randomised double-blind placebo-controlled study of the effect of Lactobacillus paracasei NCC 2461 on skin reactivity 摘要 背景/目的: 近幾十年來,工業化國家皮膚反應性受試者的患病率顯著增加。50% 的女性和 30% 的男性皮膚不適報告被歸類為反應性/敏感皮膚。目前已經出現幾種局部方法: 特別是通過改進蓋崙製劑或保護表皮表面。作者想要透過創新的營養方法從體內採取不同的行動,因此選擇副乾酪乳桿菌 NCC 2461 (ST11) 是因為其在體外研究中發現的特定有益皮膚特性,即減少神經源性炎症和促進皮膚屏障功能的恢復。 方法: 作者設計了一項隨機雙盲安慰劑對照臨床研究,隨機分配兩個組別(每組 n = 32),進行為期兩個月的補充,並在這期間進行辣椒素測試以監測皮膚敏感性。此外,還評估了經皮水分流失,以分析皮膚屏障功能恢復的速度;皮膚科醫生和自我評估對腿部乾燥和臉頰粗糙進行了調查。 結果: 本臨床試驗的結果表明,口服益生菌補充劑可降低皮膚敏感性並提高屏障功能恢復的速度。因此,數據提供了證據表明每天攝入 ST11 可以改善反應性皮膚狀況。 簡介 在工業化國家,皮膚反應性患者的數量顯著增加,大約有50%女性和30%的男性的皮膚不適症狀被歸類於反應性/敏感性皮膚。此皮膚不適的主要症狀為神經知覺,像是有熱、灼燒、刺痛或燒癢的感覺,另外,反應性或敏感性皮膚的特徵是對物理(熱、冷、風)或化學(局部應用產品)刺激有敏感的反應。在急性期,神經源性炎症可能由促炎神經介質的釋放引起。 另一方面,反應性皮膚也與皮膚屏障功能受損的恢復有關聯。許多研究指出,皮膚屏障功能在反應性皮膚起到關鍵性作用,屏障功能降低是增強潛在刺激性物質滲透性的原因。另外,皮膚經皮失水率(TEWL)所反應的表皮内穩態水合水平與皮膚屏障的狀態密切相關,因为皮膚屏障的破壞會導致TEWL的增加。而某些益生菌菌株調節免疫功能的能力是使用活菌來預防或改善皮膚過敏,特别是皮膚症狀臨床結果的基本依據。已有臨床數據顯示特定益生菌菌株(副乾酪乳桿菌),可以調節免疫穩態或下調免疫相關疾病 。 在本研究中,作者研究了口服ST11益生菌對人體反應性皮膚症狀的結果,並透過皮膚敏感性及皮膚屏障功能恢復狀態進行評估。 結果 结果表明,ST11對於皮膚敏感性和皮膚屏障功能恢復均有正向影響的结果。受試者在補充ST11後,有顯著性差異减少皮膚對辣椒素的敏感性。 作者們評估三種構成益生菌對皮膚敏感性的潛在作用機制: (1)直接作用: 通過抑制神經介質的釋放参與敏感性反應 (2)降低神經性發炎反應 (3)對皮膚屏障功能有正面影響 參考文獻 1.De Lacharrière, O., 2002. Peaux sensibles, peaux réactives.Cosmétologie et Dermatologie Esthétique 50-220-A-10. 2.Del Giudice, M., De Luca, M.G. and Capristo, C., 2002. Probiotics and atopic dermatitis. A new strategy in atopic dermatitis. Digestive and Liver Diseases 34 Suppl. 2: S68-S71. 3.Farage, M.A., Katsarou, A. and Maibach, H.I., 2006. Sensory, clinical and physiological factors in sensitive skin: a review. Contact Dermatitis 55: 1-14. 4.Gueniche, A., Benyacoub, J., Philippe, D., Bastien, P., Kusy, N., Blum,S., Breton, L. and Castiel-Higounenc, I., 2010. Lactobacillus paracasei CNCM I-2116 (ST11) inhibits substance P-induced skin inflammation and accelerates skin barrier function recovery in vitro. European Journal of Dermatology 20: 731-737. 5.Ibnou-Zekri, N., Blum, S., Schiffrin, E.J. and Von der Weid, T., 2003.Divergent patterns of colonisation and immune response elicited from two intestinal Lactobacillus strains that display similar properties in vitro. Infection and Immunity 71: 428-436.

2022.05.20
嗜酸乳桿菌LB為一種治療消化系統疾病的有用藥物本篇文章導讀自: Lactobacillus acidophilus LB: a useful pharmabiotic for the treatment of digestive disorders 摘要 菌群失調是常駐細菌群落與其宿主之間失去平衡,通常與多種疾病有關,包括炎症性腸病(非特異性慢性潰瘍性結腸炎和克羅恩病)和消化功能障礙。益生菌、益生元、合生元生物以及最近的藥生元已被證明可以調節人類微生物群。在這篇綜述中,作者重點介紹了有關一種獨特的藥生菌—嗜酸乳桿菌LB ( Lactobacillus boucardii ) 在用於治療胃腸道疾病的現有臨床證據。由於它不含活生物體,因此即使在存在免疫抑制的情況下,給予嗜酸乳桿菌LB 作為治療急性腹瀉、慢性腹瀉和抗生素相關性腹瀉的佐劑也是有效和安全的。 簡介 微生物群與人類之間的複雜相互作用目前被認為是平衡(共生)和生命發展的基礎。醫學研究表明,常駐細菌群落與其宿主之間失去平衡(生態失調)會導致多種疾病。與生態失調相關的疾病有很多,包括代謝疾病(例如肥胖、脂肪肝、心血管疾病等)、感染過程(急性腹瀉、抗生素相關性腹瀉和艱難梭菌感染)、惡性腫瘤(例如結腸癌) ,炎症性腸病(非特異性慢性潰瘍性結腸炎和克羅恩病),以及消化功能障礙(尤其是腸易激綜合徵)。 由於生態失調被認為是一種病理生理機制,因此有人提出通過藥物和食物(益生菌、益生元、合生菌和最近的藥生菌)調節微生物群可能有助於恢復益生菌狀態。此外,該主題引起了科學界和公眾的興趣。媒體上通常會聽到一些建議,宣傳使用”益生菌“作為維持健康狀況的有益措施。 必須承認,前面提到的每個術語都彼此不同,而且它們的好處的證據是異質的;這意味著並非所有這些都以相同的方式起作用,並且不應假設菌株、益生元或藥生元的作用在所有條件下都是相似的。本文詳細回顧了與胃腸道疾病相關的菌群失調相關概念,以及嗜酸乳桿菌LB菌株作為治療此類疾病的藥物的具體用途。 臨床實驗 結果 人們認識到通過飲食來維持腸道菌群非常重要,當因為疾病、抗生素使用或其他原因而出現生態失調時,益生菌可以作為營養保健品或替代藥物。目前,有足夠的證據認為嗜酸乳桿菌LB 作為治療急性腹瀉、抗菌藥相關性腹瀉和慢性腹瀉的佐劑是有效和安全的。 參考文獻 1.Petersen C, Round JL. Defining dysbiosis and its influence on host immunity and disease. 2.Cell Microbiol 2014; 16: 1024–1033. 3.Chang C, Lin H. Dysbiosis in gastrointestinal disorders. 4.Best Pract Res Clin Gastroenterol 2016; 30: 3–15. 5.Vemuri RC, Gundamaraju R, Shinde T, et al. Therapeutic interventions for gut dysbiosis and related disorders in the elderly: antibiotics, probiotics or faecal microbiota transplantation? 6.Benef Microbes 2017; 8: 179–192. 7.Adams CA. The probiotic paradox: live and dead cells are biological response modifiers. 8.Nutr Res Rev 2010; 23: 37–46 9.Salazar-Lindo E, Figueroa-Quintanilla D, Caciano MI, et al. Effectiveness and safety of Lactobacillus LB in the treatment of mild acute diarrhea in children. 10.J Pediatr Gastroenterol Nutr 2007; 44: 571–576. 11.Liévin-Le Moal V, Sarrazin-Davila LE, Servin AL. An experimental study and a randomized, double-blind, placebo-controlled clinical trial to evaluate the antisecretory activity of Lactobacillus acidophilus strain LB against nonrotavirus diarrhea. Pediatrics 2007; 120: e795–e803. 1.Simakachorn N, Pichaipat V, Rithipornpaisarn P, et al. Clinical evaluation of the addition of lyophilized, heat-killed Lactobacillus acidophilus LB to oral rehydration therapy in the treatment of acute diarrhea in children. J Pediatr Gastroenterol Nutr 2000; 30: 68–72. 1.Liévin-Le Moal V. A gastrointestinal anti-infectious biotherapeutic agent: the heat-treated Lactobacillus LB. Therap Adv Gastroenterol 2016; 9: 57–75. 1.Xiao SD, Zhang DZ, Lu H, et al. Multicenter, randomized, controlled trial of heat-killed Lactobacillus acidophilus LB in patients with chronic diarrhea. Adv Ther 2003; 20: 253–260. 1.Sniffen JC, McFarland LV, Evans CT, et al. Choosing an appropriate probiotic product for your patient: an evidence-based practical guide. PLoS One 2018; 13: e0209205.

2022.05.20
EPA魚油到底怎麼吃? 文獻證實:這幾種人適合吃高濃度EPA魚油介紹 吃魚油的好處,魚油的主要有效成分為人體無法合成的多元不飽和脂肪酸Omega-3,缺乏Omega-3會造成心血管疾病、精神疾病、腎臟疾病還有發炎及癌症相關疾病的風險。Omega-3又可分為EPA及DHA這兩種主要功效成分。市面上魚油的產品百百種,純EPA、DHA及EPA+DHA,各有不同效果,而今天將著重介紹開啟新世代魚油的大功臣: EPA! 本篇匯整了科學文獻資料,帶大家了解EPA到底是何方神聖,它的功效有哪些、誰適合吃、劑量吃多少,將在這篇為大家解答! EPA 學名為二十碳五烯酸Eicosapentaenoic acid,是屬於Omega-3系列的必須脂肪酸,主要功效有以下幾點: 降低三酸甘油脂(TG)含量 防止血管及動脈硬化 預防心血管疾病 初級預防心臟病 改善圍產期憂鬱症、重度憂鬱症及焦慮症 改善ADHD過動症 提高洗腎病患生存率、減緩搔癢症狀 提高COVID-19患者生存率、縮短感染症狀持續時間 EPA與DHA的差異 EPA適用族群與劑量 重大心血管事件高風險族群(醣尿病、三高患者)攝取純EPA 2~4g 心臟病及中風高風險族群 攝取純EPA 2g 憂鬱症 攝取純EPA 1~2g 焦慮症 攝取純EPA 2g 孕婦中晚期憂鬱症 攝取 EPA 2.2g + DHA 1.2g ADHD過動症 攝取純EPA 0.5g~1.2g IgA腎病變 攝取純EPA 2~4g 心血管疾病與EPA的關係 服用EPA可以降低高危險群(如:膽固醇過高、糖尿病患者)造成心血管事件的風險 身心疾病與EPA的關係心血管疾病與EPA的關係 國際營養精神病學學會建議 治療重度抑鬱症用量應為每天 1-2 克 EPA。EPA可降低血液中的發炎因子,改善憂鬱焦慮等症狀,除此之外,有報導指出EPA對於過動症(ADHD)也有治療效果。 洗腎病人與EPA的關係身心疾病與EPA的關係 慢性腎臟病會增加心血管疾病的風險,包含過高LDL-C、三酸甘油脂及動脈粥狀硬化等等,有將近60%的腎臟病患者有尿毒搔癢的症狀。 研究證實,服用足量EPA有效提高慢性腎臟病患者的存活率且減少尿毒搔癢症狀。 洗腎病人與EPA的關係 COVID-19與EPA的關係 服用EPA有效減少COVID-19病患症狀持續時間,改善腎功能及呼吸等多項參數水平,並提高重症病患的七倍存活率 COVID-19與EPA的關係 總結 高濃度EPA適合有以下特殊疾病需求做為日常預防保健

2022.04.30
如何挑選魚油相信大家對於魚油一定不陌生吧!但魚油從哪裡來?裡面到底又有什麼成分呢?魚油的功效是什麼?下面就由我們來揭開魚油的神秘面紗吧! 何謂魚油? 魚油是從魚身上所提取出來的油脂,通常會從鯡魚、鯖魚、鮭魚及沙丁魚等等…這些富含高油脂的魚類萃取出油脂。那麼多吃魚能不能攝取到魚油呢?答案是可以的,不過現代人外食多、飲食不正常,要達到美國心臟協會所建議的攝取量”每周攝取兩次100克油脂較多的魚”大多不太容易,再加上魚類來源是否安全、是否有受到重金屬汙染,也是需要考慮的問題。 魚油的類型 魚油常見的有三種類型,分別為EE Form、TG Form以及rTG Form EE Form為酯化型魚油,萃取出魚油後再經分子蒸餾法酯化,將甘油分子以乙醇替換,分離出其中的多元不飽和脂肪酸及環境毒素。EPA+DHA濃度可高到50-70%。 TG Form為三酸甘油脂型,萃取魚的皮下脂肪,稍微精煉去除雜質,仍保持天然魚肉皮下脂肪結構。EPA+DHA的濃度約30%。 rTG Form為三酸甘油脂型,是加工濃縮提高濃度之後,再將酯化型魚油還原成三酸甘油脂的型態,EPA+DHA濃度可維持50-70%。 EE Form及TG Form這兩種魚油在製造過程的差別在於TG Form魚油是在腸道內經脂肪分解酵素(Pancreatic Lipase)分解,EE Form是在腸道內皮細胞(Endothelial Cells)被分解,所以TG Form短時間的吸收速度會比較快,EE Form則為緩慢釋放以維持穩定的omega 3濃度。根據Dyerberg J博士發表之n-3脂肪酸的生物利用度之論文,TG Form和EE Form之最終吸收率極為相近。 魚油的萃取方法 常見的萃取方法有幾種:水煮法、分子蒸餾法及二氧化碳超臨界萃取法 水煮法,為最傳統的萃取方式,製作過程因容易接觸到空氣加上經由高溫加熱,油脂氧化的機率很高,容易產生油耗味,因此現今已經比較少使用。 分子蒸餾法(molecular distillation),在低蒸氣壓的環境中,對於熱不穩定物質的分離、純化和濃縮有良好效果。利用低溫真空狀況來移除魚油中的有害物質,同時達到防止魚油氧化和酸敗。 超臨界萃取法,又稱超臨界流體萃取Supercritical Fluid Extraction (SFE),通常使用二氧化碳作為流體萃取劑,把魚油有效成分從酯化型魚油中分離出來,去除魚油中不需要的物質,包含重金屬等汙染物。 魚油的營養組成 魚油由上百種脂肪酸所組成,包含不飽和脂肪酸(Omega3、6)及飽和脂肪酸(Omega 9),其中Omega-3為人體無法自行合成的必需脂肪酸,需要額外攝取。Omega-3主要營養素為二十碳五烯酸 (eicosapentaenoic acid,EPA) 和二十二碳六烯酸 (docosahexaenoic acid,DHA),是被研究證實有功效的主要成分。 美國心臟協會期刊《Stroke》研究指出 二十碳五烯酸 (eicosapentaenoic acid,EPA) 可減少低密度脂蛋白膽固醇、三酸甘油脂的含量,進而保護心血管、防止血栓。另外國際醫學期刊《心理治療與身心醫學》 研究指出有助於身心疾病等功效。 二十二碳六烯酸 (docosahexaenoic acid,DHA)則被證實與大腦營養、認知及眼睛健康有關。 魚油的挑選法則 市面上充斥著許多魚油保健食品,挑選符合個人需求且品質良好的魚油顯得更為重要。主要可以分成兩大部分,分別為需求及魚油品質: 需求:市面上大多為EPA/DHA混合型式的魚油,在上述魚油營養組成中有提到EPA及DHA實際上分別扮演著不同角色,其主要功能也不同,因此在挑選魚油時應該先根據自己想要改善哪方面的問題,對症下藥,補充魚油才會有效果。 EPA: 降低低密度脂蛋白膽固醇、三酸甘油脂含量或預防心血管疾病: 目前有大型研究證實純EPA與Statin類藥物合併使用可降低25%心血管事件發生率。另外,DHA+EPA有可能會導致低密度脂蛋白膽固醇上升,因此不建議吃含有DHA的魚油。 圍產期憂鬱症、重度憂鬱症身心相關保健: 根據《心理治療與身心醫學》期刊及2019年國際營養指引建議每天投予1-2克的EPA,或是每天投予1-2克的EPA與DHA (比例應大於2:1),可以改善重度憂鬱症。 ADHD過動症: 2018年發表在神經精神藥理學雜誌的研究發現EPA>500對於ADHD行為得到改善 。 DHA: 孕期胎兒營養補充: 母體 DHA 攝入量和循環 DHA 濃度決定胎兒血液DHA濃度 。 眼睛健康保健: 參與視覺和神經功能以及神經遞質代謝。 大腦營養補充: 維持思緒清晰及專注力。 DHA+EPA: 孕婦延長姙娠期: 研究證實食用Omega 3可以降低早產機率,<37周早產率降低11%,<34周早產率降低42%。 2. 魚油品質: Omega 3濃度>80%以上: 須留意魚油Omega-3(EPA+DHA)的濃度是否清楚標示,經研究證實>80%的Omega-3有更高的吸收率且有效降低三酸甘油脂(TG)及低密度脂蛋白(LDL)。 重金屬檢測報告: 吃魚油最害怕的就是有重金屬污染的問題,因此有重金屬檢驗報告的魚油對於消費者來說會相對更有保障。 魚油清澈程度: 與萃取技術有關,魚油外觀若看起來越清澈代表雜質越少、萃取技術越好。 魚油與維生素D一起食用 在2021/11 /3 至 10 日所舉行的美國風濕病學會 (ACR) Convergence 2021 上公佈的研究指出:補充維生素 D3 和 omega-3 脂肪酸可使老年人患自身免疫性疾病的風險降低 25% 至 30%。 魚油如何吃? 魚油屬於油脂類,建議在用餐時或飯後食用較佳,因為食物中的脂肪有助於脂溶性維生素的吸收。 食用魚油的注意事項 對海鮮、魚類過敏者,建議避免食用。 過去魚油被認為與凝血功能有相關性,如近期有需要開刀或孕婦,會建議暫停使用。不過近期的文獻指出魚油並不會影響凝血功能,且另有研究指出圍產期食用高濃度EPA魚油可改善圍產期抑鬱症及延長姙娠期,預防早產。因此孕婦在32周之後如要食用魚油可以先詢問專業醫事人員建議以及檢查凝血相關功能再進行食用。 小結 吃對比吃多更重要! 根據自己的需求及魚油品質的鑑別選擇最適合自己的魚油才是正確的消費行為 因為魚油需要長期食用,因此不論是選擇TG Form還是EE Form,長久來看其最終吸收率並無明顯差別

2021.06.07
漫談益生菌與人體健康林口長庚胃腸科臨床教授 陳邦基 西元1905年俄國微生物學家梅契尼可夫(Metchnikoff)觀察保加利亞人瑞每天有飲用酸奶的習慣,推論酸奶中之乳酸菌有抑制腸道害菌、延緩老化作用,認為「老化始於腸」、倡導「乳酸菌長壽說」。他在1908年得到諾貝爾獎,後人因其畢生提倡乳酸菌對健康的好處,尊稱為「乳酸菌之父」,並設立「梅契尼可夫獎」紀念其貢獻。近代的日本東大光岡知足教授就曾榮獲此獎,並且經過一世紀的研究,得知長壽人瑞的腸道中雙歧桿菌比一般人要高60至100倍,確立了「微生物介入治療」的概念,證實了補充益生菌可改善人體健康的理論。 腸道的細菌 人類腸道內的細菌數目高達百兆以上,總共500多種,重量超過1公斤,而且70%以上的免疫細胞都在腸道,所以腸道是人體最大的免疫器官。腸道共生菌與人體宿主基因共同演化,互相整合,形成和平共存、共生互利的所謂「人體超級生物體」,因而腸內細菌也可看成是一種器官,且是十大必要器官之一。腸道免疫系統包括淋巴組織,培爾氏斑(Peyer` patch)、淋巴球、巨噬細胞、樹突細胞、B細胞、T細胞、自然殺手細胞等,共同形成一道防線,防止病原入侵。腸道細菌有99%在大腸(1公克有百、千億菌),迴腸次之(1公克有10億菌),空腸(1公克有千、萬菌),胃及十二指腸最少(1西西有百、千菌量)。腸菌對人有好有壞,好菌佔10~20%,其發酵作用能將醣類、寡糖及纖維質代謝分解為乳酸、醋酸、二氧化碳及氫氣。而壞菌佔20%,有腐敗作用,會將蛋白質、脂肪代謝產生氨、硫化氫、酚、亞胺,產生臭味、毒素,使人腹瀉、便秘、老化、生病、致癌。中性菌佔60~70%,平時不好不壞,免疫力低或生病時則變壞,屬騎牆派性質,牆頭草一般,可以變成好菌,也可以變成壞菌,端視何者佔上風而靠攏,故有伺機菌之稱。 益生菌Probiotic 益生菌對宿主、人體有益,是可改善腸道菌相的活菌微生物。最具代表性益生菌─乳酸菌,能分解醣類(乳糖、葡萄糖、蔗糖、果糖)產生乳酸和醋酸,可酸化腸道環境,抑制害菌增殖,調整腸內菌叢平衡,改善消化環境,促進腸道蠕動,提升免疫機能,預防過敏,抑制感染,增加酵素、維生素和干擾素的合成。乳酸菌包括乳酸桿菌、雙歧桿菌、酵母菌及其他桿菌、球菌等。 好菌(益菌) 益生菌就是好菌,包括(1)乳酸桿菌(Lactobacillus),較常被提及的有嗜乳酸桿菌(A菌)、乾酪(凱氏)菌(C菌)、LGG、代田菌、LP33、LG21、LS菌、植物、洛德氏、短乳酸桿菌、保加利亞菌(LB)、嗜熱鏈球菌(ST)、脆弱類桿菌及宮入菌等。(2)雙歧桿菌(Bifidobacterium),包括比菲德氏菌(B菌)、龍根、雷特氏、短雙岐桿菌等。因長壽者腸內B菌特多,也被稱為長壽菌。(3)布拉氏酵母菌(Saccharomyces boulardii)(4)乳酸腸球菌(Enterococcus faecalis)(5)生存於陰道的乳酸桿菌,可維持陰道PH值在3.5至4.5間,防止白色念珠菌感染,也被稱為Doderlein` bacillus。 壞菌(害菌) 壞菌包括產氣莢膜桿菌(魏氏梭菌)、困難腸梭菌、金黃色葡萄球菌、病原性大腸桿菌、綠膿桿菌、克雷白氏菌、沙門氏菌和志賀氏菌等。 中性(中間)菌 包括糞鏈球菌、非病原性大腸桿菌、腸球菌、脆弱類桿菌、厭氧性鏈球菌、酵母菌、黴(真)菌、麴菌和優桿菌(真細菌)等。 益菌生Prebiotics 透過飲食的補充,可增加腸內益菌的生長(養菌作用),也叫益菌素、益生元(源)、益生質或益生菌助生質。包含寡糖、膳食纖維及一些中草藥。寡糖(低聚糖Oligosaccharides, OS):只有B菌可以利用的食物,有半乳寡糖、果寡糖、木寡糖、異麥芽寡糖、大豆寡糖、乳果寡糖、異果寡糖、菊糖等,來源為母奶、豆類、根莖類、全穀、海藻、蔬果、蕈菇、蜂蜜等食物。(2)膳食纖維(Dietary fiber):益害菌皆可利用。亦稱為第六(七)大營養素。包括(a)水溶性:果膠、植物膠、海藻酸、褐藻糖膠、昆布多醣、黏質物、菊苣纖維、葡甘露聚醣等,來源為熟水果、種子、根莖、海藻等。(b)非水溶性:果膠(未熟蔬果)、纖維素、半纖維素、木質素、甲殼素、聚葡萄糖等,來源為穀類、蔬菜、豆類、未熟水果、麩皮、牛蒡、蘑菇、蝦蟹殼等。膳食纖維成人攝取量每天為15至30公克(25公克以上較好)。(3)中草藥(Herbs):人蔘、枸杞、靈芝、茯苓、當歸、刺五加、何首烏。 合益素(合生元、合生素) Synbiotics 益生菌與益菌生之結合,可以稱為大腸的食物。最初是以牛奶初乳加上益生菌製成寡糖乳酸菌,有保胃整腸,平衡腸道菌叢(增加B菌、減少害菌),抑制腸內有害物質,增加免疫功能,預防腸道感染,抑制害菌減少癌症,調整過敏體質,預防陰道感染之功用。 益生菌生成萃取物(益生素) Biogenics 乳酸菌生成萃取液乃是利用多種共生乳酸菌,以有機大豆豆漿為培養基,經過一年熟成,再以高科技萃取有效分泌物及菌體物質而製成。分泌物的功能為活化定居菌之酵素,抑制害菌,促使中性菌變成益菌,增進益菌繁殖,稱為養菌。而菌體物質的作用為活化免疫細胞,修護腸道細胞。市面上有ALBEX、Lactis(日)、Lacteol(法)等成品問世。

2021.06.03
有關胃腸道的細菌性毒素之發表口服活性碳會吸附腸道內有毒物質, 本身不被人體吸收,過去是使用在緊急治療藥物或化學品中毒之病人。 近年來的研究發現活性碳會吸附干擾胃腸道的細菌性毒素、消化性毒素及其他有機性廢物、解除腸內滯留氣體及有關症狀。 還有實驗證明某些 特殊劑型的口服活性碳 (例如: 多孔分散吸附元、微球細粒吸附碳等), 可在腸胃道選擇性的吸附重金屬、indole及p-cresol,以減少人體吸收的機會,進而延緩慢性腎衰竭患者透析起始時間及改善尿毒症狀。

2021.06.03
~歡迎踴躍申請網路會員~~歡迎踴躍申請網路會員~另 申請時請務必確實填寫相關資訊,以利完成申請程序審核~協會有保留 會員申請核准與取消資格之權益~ 本協會將會不定期舉辦專業主題研討會,敬請期待與參與~~

2021.06.03
認識「健康體能」民眾也許感到很疑惑,以往聽過「體適能」,現又有「健康體能」,二者究竟有何不同呢?「體適能」(Phyical fitness) 是國內體育界沿用已久的名詞,事實上包含兩大類,一為 「與運動競技有關的體適能」(Sport-related fitness),另一為「與健康有關的體適能」(Health-related fitness),本署關心的是與民眾健康有關的體適能,因此稱之為 「健康體能」。以後,並將沿用本名詞推展各相關業務,以促進民眾健康。 二、「健康體能」的涵意 所謂「健康體能」是指人的器官組織如心臟、肺臟、血管、肌肉等都能發揮正常功能,而使身體具有勝任日常工作、享受休閒娛樂及應付突發狀況的能力。 人的體能狀況可經由測量得知,且可利用規律活動或運動來改進,本署期待國民均有健康的身體及適當的體能,因此將利用本書介紹成年人評估健康體能的方法,並提出適當的運動建議。 三、健康體能的四大要素 (一) 心肺耐力 為健康體能四大要素中最重要的一項,其所涉及的範圍包括:心臟、肺臟、血管及血液等器官組織系統的機能。 運動生理學家和醫學研究者都已一致證實心血管循環耐力是體能評量的最重要指標。 (二) 肌力與肌耐力 肌耐力經常被人誤以為是肌肉力量,其實肌肉力量代表的是某一部位的肌肉或肌群一次能發揮的最大力量,而肌肉耐力則是某一部位肌肉或肌群在從事反覆收縮動作時的一種持久能力;或是指有關的肌肉維持某一固定用力狀態持久的時間而言。 肌力與肌耐力的訓練可以使肌肉纖維變粗,除了增加本身所能發出的力量外,也增強肌肉的耐久能力。身體任何大小的動作都是靠著肌肉牽引骨骼而完成的,肌肉本身若無法發出適當的力量,有些動作會顯得相當吃力或無法完成,也容易產生肌肉疲勞。很多成年人患有下背部疼痛,身體肌力不足是主要的原因之一。 (三) 柔軟度 這種能力代表的是人體的關節可以活動的最大範圍。而真正影響柔軟度的因素除了骨骼本身的結構外,還有肌肉、肌腱、韌帶、軟骨組織等。較佳的身體柔軟度表示肢體軀幹在運動、彎曲、伸展、扭轉時都比較輕鬆自如,同時也可以使肌肉與韌帶受到較好的保護而免於因受力而受傷。 (四) 身體組成(身體脂肪百分比) 從健康的觀點,肥胖是威脅生命的高危險因子,與心臟病、高血壓、膽囊疾病、糖尿病、肺活量減少、高脂血症及骨骼關節的疾病都有很密切的相關。因此身體脂肪百分比也是評估健康體能的重要項目,隨著文明的進步和生活水準的提昇,人類身體活動的機會減少,而熱量攝取常超越身體所需,使肥胖日漸增加。因此,要保持身體適當的脂肪百分比,除了需要均衡飲食外,更需要加強運動,藉以燃燒脂肪消耗身體過剩熱量,同時亦是達成體重控制的良好方法。 四、體能與健康的關係 現代社會以機器取代人力,因此一般工作與日常生活只需要普通的體能即可勝任,那麼,為什麼要提倡健康體能呢?事實上,一個人的體能狀況與生活品質和健康有密切的關係。 體能的衰退對個人有雙重影響,第一、年紀愈大,如果體能很差,常不足以應付日常活動之所需,因而無法獨立生活,生活品質低落,第二、體能衰退與缺乏運動息息相關,而缺乏運動又是危害健康的重要危險因子。 一般人的心肺耐力(以最大攝氧量代表),自25歲以後,每年約減少 1%,因此到了75歲時,心肺耐力可能只有年輕時的一半。此外,體脂肪由青年到中年迅速增加,肌肉量由中年至老年則迅速減少。 而缺乏運動者與經常運動者比較,罹患冠狀動脈心臟病的機會增加1.5至2.4倍,發生糖尿病的機會增加2至4倍,得到大腸癌的機會則增加2至5倍,據估計如果全民均從事適當運動,人口中因上述疾病而死亡的人可以減少三分之一。此外,缺乏運動與高血壓、高脂血、骨質疏鬆都有密切關係。 推廣健康體能活動有兩個好處,對個人而言,可提昇個人對自我體能狀況及適當運動重要性的認知,進而培養規律運動的習慣,以促進個人的健康體能,提高生活品質,並減少因缺乏運動而產生之退化性或慢性疾病的發生,延長健康的壽命。對社會而言,可有效提昇全民身體活動量,以促進國民健康體能狀況,進而提昇國家競爭力,節省醫療支出,減少中高年齡人口對社會及家庭的負擔。 能
2021.04.02
學術分享 Blood omega-3 fatty acids and death from COVID-19: A pilot studyProstaglandins, Leukotrienes and Essential Fatty Acids Volume 166, March 2021, 102250 Short communication Blood omega-3 fatty acids and death from COVID-19: A pilot study Author links open overlay panelArashAsheraNathan L.TintlebcMichaelMyersdLauraLockshonaHeribertBacarezaeWilliam S.Harrisbf a Samuel Oschin Comprehensive Cancer Institute at Cedars-Sinai Medical Center, Los Angeles, CA b Fatty Acid Research Institute, Sioux Falls, SD c Department of Mathematics and Statistics, Dordt University, Sioux Center, IA d Los Alamitos Medical Center, Los Alamitos, CA e Department of Medical Affairs, Cedars-Sinai Medical Center, Los Angeles, CA f Department of Internal Medicine, Sanford School of Medicine, University of South Dakota, Sioux Falls, SD Received 6 January 2021, Revised 17 January 2021, Accepted 17 January 2021, Available online 20 January 2021. Show less Add to Mendeley Share Cite https://doi.org/10.1016/j.plefa.2021.102250Get rights and content Highlights • Nutrition-based interventions to reduce COVID-19 morbidity/mortality are needed. • The Omega-3 Index (O3I) was measured in banked blood from 100 COVID-19 patients. • Risk for death was analyzed as a function of quartiles (Q) of the O3I. • Patients in Q4 (O3I ≥ 5.7%) vs. Q1–3 were 75% less likely to die (p = 0.07). • These pilot data suggest that a higher O3I may lower risk for death from COVID-19. Abstract Very-long chain omega-3 fatty acids (EPA and DHA) have anti-inflammatory properties that may help reduce morbidity and mortality from COVID-19 infection. We conducted a pilot study in 100 patients to test the hypothesis that RBC EPA+DHA levels (the Omega-3 Index, O3I) would be inversely associated with risk for death by analyzing the O3I in banked blood samples drawn at hospital admission. Fourteen patients died, one of 25 in quartile 4 (Q4) (O3I ≥5.7%) and 13 of 75 in Q1–3. After adjusting for age and sex, the odds ratio for death in patients with an O3I in Q4 vs Q1–3 was 0.25, p = 0.07. Although not meeting the classical criteria for statistical significance, this strong trend suggests that a relationship may indeed exist, but more well-powered studies are clearly needed. Previous article in issue Next article in issue Keywords Omega-3 fatty acids Eicosapentaenoic acid Docosahexaenoic acid COVID-19 Total mortality Omega-3 index Inflammation 1. Introduction COVID-19, the illness caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has been diagnosed in over 80 million people worldwide as of the end of 2020, and over 1.8 million have died [1]. Although 81% of symptomatic individuals have relatively mild disease, 14% will develop severe disease characterized by dyspnea, hypoxia, or >50 percent lung involvement by imaging, with the remaining 5% developing critical disease characterized by respiratory failure, shock, and/or multiorgan dysfunction [2]. Severe and critical disease from COVID-19 is associated with advancing age (especially over 65 years), male gender, chronic lung disease, obesity, cardiovascular disease including hypertension, diabetes, and other chronic medical conditions. Severe COVID-19 disease and death is, in part, mediated by rapid elevations of inflammatory cytokines including TNF-alpha, IL-1β, and IL-6 leading to a cytokine release syndrome or “cytokine storm.” [3] Accordingly, an attractive preventative approach to COVID-19 infection is to minimize cytokine release. Very long-chain omega-3 s (DHA and EPA) found in fish oils have a plethora of biological activities including directly and indirectly modulating inflammatory responses and cytokine release [4], [5], [6]. In non-COVID-19 ettings, higher intakes [7], [8] and blood levels [9], [10] of these omega-3 s are associated with lower levels of circulating inflammatory cytokines, and intervention with fish oils reduces levels [11], [12]. EPA and DHA are precursors to a suite of inflammation-resolving mediators (IRMs; resolvins, maresins and protectins [13]) that actively regulate the resolution of acute inflammation. IRMs down-regulate cytokine production and promote a return to homeostasis via monocyte/macrophage-mediated uptake of debris, apoptosis of neutrophils, and clearing of microbes. Accordingly, higher intakes of EPA and DHA (which result in higher RBC EPA+DHA levels, hereafter called the Omega-3 Index, O3I [14], [15]) have been proposed to lower the risk for adverse outcomes from COVID-19 [16], [17], [18], [19], [20], [21], [22], and case reports suggesting benefit have been published [23], [24]. Given the profound public health concerns related to the current COVID-19 pandemic, modifiable risk factors for developing severe and critical complications are urgently needed, especially ones that may be easily implemented and nutritionally based. Despite the known mechanisms by which IRMs and omega-3 fatty acids support the active, endogenous resolution of inflammatory mechanisms, to our knowledge no study has explored the relationship between omega-3 tissue levels and COVID-19 outcomes. The primary objective of this pilot study was to define the relationship between O3I and death from COVID-19. We hypothesize that a higher O3I is associated with lower risk for death in these patients. 2. Methods 2.1. Subjects We studied 100 patients hospitalized at Cedars-Sinai Medical Center from March 1, 2020 onwards with confirmed COVID-19 infection who met the criteria for inclusion, which were the availability of basic demographic data, clinical outcomes and an EDTA blood sample (drawn within 10 days of diagnosis) stored at −80 °C at the Cedars-Sinai biorepository. If more than one sample was available, the first sample drawn after the time of diagnosis was utilized. We utilized sample remnant protocol Pro00036514 to obtain blood samples for this study. Briefly, a protocol was submitted to the Enterprise Information Service (EIS) team and staff members of the Biobank. After review and approval, the EIS/Biobank team pulled the samples and the data, de-identifying each sample by assigning a study-specific number. Using this protocol, we obtained a limited data and blood sample set to conduct this pilot investigation. The study was approved by the IRB of Cedars-Sinai Medical Center (STUDY-00,000,779). 2.2. Clinical outcomes The primary outcome was death from COVID-19 infection. 2.3. Laboratory Blood samples were thawed at the biorepository and one drop was placed on a dried blood spot collection card pre-treated with antioxidants to protect the fatty acids from degradation. The cards were then shipped overnight in batch to OmegaQuant Analytics (Sioux Falls, SD) for analysis of fatty acids and calculation of the Omega-3 Index [25]. Briefly, blood spots were transferred to a reaction vial and FA methyl esters (FAMEs) were generated using boron trifluoride in methanol by heating for 45 min at 100 °C. FAMEs were extracted into hexane (after the addition of water) and analyzed using a GC2010 Gas Chromatograph (Shimadzu Corporation, Columbia, MD) equipped with a SP2560, 100-m column (Supelco, Bellefonte, PA). FAMEs were identified by comparison with a standard mixture (GLC, Nucheck Prep, Elysian, MN). Analysis was conducted using an internal-standard-based, three-point calibration curve to quantify levels of 24 FAMEs which were each expressed as a percent of total FAs. The O3I was calculated from the dried blood spot EPA+DHA value as described previously [25]. The analytical coefficient of variation for the O3I is <5%. 2.4. Statistical methods The study sample is described using standard descriptive statistics (means and standard deviations, medians and ranges, and counts and percentages). Additional descriptive summary of the sample is provided by stratifying using quartiles of the O3I or by comparing Q4 to Q1–3. The distribution of age, sex and do not resuscitate (DNR) status by O3I quartiles or top 25%/bottom 75% was tested using an F-test (age) or Chi-squared test (sex, DNR status). The primary analysis examined the hypothesis that O3I is associated with risk for death. We first predicted death using unadjusted logistic regression models by quartiles of the O3I using a Chi-squared test to evaluate overall (4-group) association. We also predicted death by age, sex and DNR status to evaluate and confirm known associations between risk for death and these factors. Subsequently, significant association between O3I quartiles and death was tested using logistic regression and by comparing Q4 with Q1–3 in both unadjusted models and models adjusted for age and sex. To account for the small sample sizes present in this study, primary model results use Firth's adjustment for small sample sizes in logistic regression using the logistf package in R [26]. We also report conventional logistic regression F-test results for comparison. A 2-tailed p-value of 0.05 was used for statistical significance. 3. Results 3.1. Sample description The study sample is described in Table 1. They were predominantly men, the mean age was over 70, and they were admitted between April and July 2020. Nearly 40% were under a DNR order instituted at some point during the hospitalization, and 14% died during hospitalization. The average O3I was 5.09%, and the median was 4.75%. Table 1. Descriptive statistics. Characteristics of sample % (X/N) or Mean (SD; min,max) Sex – Male 59% (59/100) Age 72.5 (16.5; 25,100) Month of data collection April – 47% (47/100) May – 25% (25/100) June – 15% (15/100) July – 13% (13/100) Red blood cell EPA+DHA (% of RBC fatty acids; the Omega-3 Index, O3I) 5.09% (1.62%; 2.87%, 13.79%) Died 14% (14/100) DNR orders 38% (38/100) Table 2 illustrates the association of the O3I by age, sex and do not resuscitate (DNR) status. Higher O3I values were significantly related to older age, with the highest mean age in the third quartile (79.8 years). Men and those who were not DNR tended to have higher O3I values, but these trends were not statistically significant. Table 2. Demographic profile of participants by category of the O3I. Categorical by O3I Quartile Age Mean (SD) Sex - Male% (x/n) DNR% (x/n) Q1 (O3I<4.0%) 63.0 (18.9) 64% (16/25) 44% (11/25) Q2 (4.0%<O3I<4.7%) 71.0 (16.1) 56% (14/25) 28% (7/25) Q3 (4.7<O3I<5.7%) 79.8 (13.3) 52% (13/25) 52% (13/25) Q4 (O3I≥5.7%) 76.3 (12.7) 64% (16/25) 28% (7/25) P-valuea 0.0014 0.77 0.20 Comparing O3I Q4 vs Q1–3 Q1–3: O3I<5.7% 71.3 (17.5) 57.3% (43/75) 41.3% (31/75) Q4: O3I≥5.7% 76.3 (12.7) 64% (16/25) 28% (7/25) P-valuea 0.19 0.56 0.23 a F-test (age and O3I) or Chi-square test (sex, DNR and O3I). 3.2. Unadjusted analyses Relationships between omega-3 status and fatal outcomes are shown in Table 3. As expected, older patients and those under a DNR order were more likely to die. In O3I Q4, there was one death (a 66-year-old male under a DNR order), whereas there were 13 deaths among the 75 patients in Q1–3. In the unadjusted model (and focusing on the small-sample size p-values), there was a significant difference in risk for death across quartiles of the O3I (p = 0.047), with those in the highest O3I quartile (Q4) having an odds ratio (OR) of 0.39 (p = 0.34) relative to Q1. In an unadjusted comparison between Q4 and Q1–3, the OR for death in Q4 was 0.28 (p = 0.11) or 3.6-fold higher (1/0.28) higher risk in Q1–3 vs. Q4. For comparison, the risk for death from COVID-19 associated with being 1-decade older was about 1.3-fold higher (p = 0.14). Hence, a low O3I appeared to be at least as predictive of risk for death as being 10-years older. The higher OR for death in Q3 was largely accounted for by age as the mean age in Q3 was the highest of all. The OR in Q3 was markedly attenuated in the adjusted analysis (Table 4). Table 3. Unadjusted associations of the Omega-3 Index and demographic variables with death. Risk factor Death% (x/N) Unadjusted Models OR (95% CI)a Firth's test P-valuea F-test P-valueb Female 14.6% (6/41) 1.00 Male 13.6% (8/59) 0.90 (0.30, 2.83) 0.85 0.88 Age Per decade – 1.33 (0.92, 2.08) 0.14 0.13 DNR Yes 34.2% (13/38) 21.76 (4.90, 206.44) <0.0001 0.001 No 1.6% (1/62) Categorical by O3I Quartile Overall model F-test 0.047 0.03 Q1 (O3I<4.0%) 12.0% (3/25) 1.00 Q2 (4.0%<O3I<4.7%) 8.0% (2/25) 0.68 (0.11, 3.86) 0.66 0.64 Q3 (4.7<O3I<5.7%) 32.0% (8/25) 3.13 (0.82, 14.30) 0.10 0.10 Q4 (O3I≥5.7%) 4.0% (1/25) 0.39 (0.04, 2.61) 0.34 0.32 Comparing O3I Q4 vs Q1–3 Q1–3: O3I<5.7% 17.3% (13/75) 1.00 Q4: O3I≥5.7% 4.0% (1/25) 0.28 (0.03, 1.26) 0.11 0.13 Bold and italics is used for p-values less than the significance level of 0.05. a Using the Firth's modified score procedure for small sample sizes. b Standard F-test from Logistic Regression ignoring small sample sizes. Table 4. Associations of the omega-3 index with death adjusted for age and sex. Risk factor Adjusted Models OR (95% CI)a Firth's test P-valuea F-test P-valueb Categorical by O3I Quartile Overall model F-test 0.078 0.0499 Q1 (O3I<4.0%) 1.00 Q2 (4.0%<O3I<4.7%) 0.58 (0.09, 3.35) 0.54 0.52 Q3 (4.7<O3I<5.7%) 2.18 (0.52, 10.80) 0.29 0.28 Q4 (O3I≥5.7%) 0.30 (0.03, 2.08) 0.22 0.22 Comparing O3I Q4 vs Q1–3 Q1–3: O3I<5.7% 1.00 Q4: O3I≥5.7% 0.25 (0.03, 1.11) 0.071 0.099 Bold and italics is used for p-values less than the significance level of 0.05. a Using the Firth's modified score procedure for small sample sizes. b Standard F-test from Logistic Regression ignoring small sample sizes. 3.3. Adjusted analyses In models adjusted for age and sex (Table 4), the overall relationship across quartiles became somewhat weaker (i.e., from p = 0.047 to 0.078), although the OR at Q4 (vs Q1) decreased slightly (0.39 to 0.30; p-value also decreased somewhat from 0.34 to 0.22). Comparing Q4 to Q1–3, the OR decreased slightly (from 0.28 to 0.25), and the p-value also decreased from 0.11 to 0.07. An OR of 0.25 implies that risk for death in COVID-19 patients with an O3I >5.7% was ~75% less than it was for patients with an O3I<5.7%. 4. Discussion The 2020 COVID-19 pandemic has had devasting effects on morbidity and mortality worldwide. While vaccines may soon slow the spread and drugs may help diminish the adverse effects of infection, preventative measures – ideally ones that are cheap, safe, and readily accessed by large numbers of people – that modulate the most severe disease outcomes are desperately needed. Some evidence is accumulating for a potential benefit of vitamin D [27], and here we examined another nutrient, omega-3 fatty acids, which like vitamin D, have multiple anti-inflammatory effects and may also reduce risk for adverse COVID-19 outcomes. In this pilot study we compared the associations between the O3I and risk for death from COVID-19 in 100 patients. We found (in age and sex-adjusted models) that those patients with an O3I at 5.7% or greater were at about 75% lower risk for death compared with those below that value (p = 0.071). Although not meeting the criteria for classical statistical significance, this strong trend suggests that a relationship may indeed exist, but more well-powered studies are clearly needed. The OR for death was higher in Q3 than in the other quartiles including Q4. Part of the reason for this was the mean age (and the percent of patients with DNR orders) was the highest in Q3. Accordingly, in the age-adjusted model the OR in Q3 dropped by a third. The comparison of Q4 to Q1–3 has historical precents. For example, in the Framingham Heart Study, significantly larger brain volumes and better cognitive function were observed in Q4 vs Q1–3 [28], and 10-year risk for dementia was 47% lower in subjects with omega-3 levels in Q4 vs Q1-Q3 [29]. More generally, higher omega-3 FA blood levels have been associated with the better clinical outcomes for cardiovascular disease [30,31], post-MI cardiac remodeling [32], telomere attrition [33], attempted suicide [34] and total mortality [35]. These data suggest that in some settings there may be threshold effects of the O3I. This study used the O3I as a biomarker of omega-3 FA status. This RBC-based metric has advantages, particularly in the acute hospitalization setting. This is because, much like a hemoglobin A1C versus plasma glucose, the O3I is a better long-term reflection of tissue omega-3 levels versus plasma omega-3 levels [36], and it would thus be less affected by an acute change in omega-3 intake, as might happen with hospitalization for an acute illness [37]. The O3I has been validated [25] and used in several interventional [14] and prospective cohort studies such as the Framingham Heart Study [31] and the Women's Health Initiative Memory Study [38]. The O3I is also easily modified by increasing the intake of oily fish (e.g., salmon, herring, mackerel, albacore tuna, etc.) which are rich in EPA and DHA, and dietary supplements of omega-3 will also raise levels [15]. The average O3I in this study was 5.1% which is similar to that seen other US-based studies [39], [40]. We also examined the associations between risk for death and EPA and DHA individually and with the omega-6:omega-3 ratio. We found the same directional relationships as with the O3I but they were not as statistically strong (data not shown). Multiple randomized clinical trials (RCTs) are currently (as of January 2021) underway testing the hypothesis that treatment with omega-3 fatty acids (EPA and DHA) will have beneficial effects on a variety of aspects of COVID-19 infection. Although their outcomes are not yet known, there are compelling scientific reasons to expect that these studies will be positive (and these same reasons formed the foundation for the present study). The data supporting a possible beneficial role for omega-3 fatty acids in COVID-19 infection come from past epidemiological, interventional, therapeutic, and basic science studies. For example, in the Framingham Offspring study [41], the O3I was inversely associated with 10 separate inflammatory biomarkers (e.g., CRP, IL-6, ICAM-1, LpPLA2, TNF receptor 2, and osteoprotegerin). In intervention studies [11], EPA supplementation alone (3 g/d for 10 weeks) significantly reduced the expression of TNFα from LPS-stimulated monocytes as did a similar dose of DHA which, in addition, lowered IL-6 and MCP-1. EPA+DHA supplements had similar effects [42]. Meta-analyses of multiple RCTs confirmed that treatment with omega-3 fatty acids routinely lowers cytokine levels [43], [44], [45]. More important than studies of effects on intermediate markers are clinical findings from RCTs. Langlois et al. [5] summarized the results of 12 RCTs of omega-3 treatment in 1280 intensive-care-unit patients with acute respiratory distress syndrome. There was a significant improvement in measures of blood oxygenation in the treated patients and strong trends (p ≤ 0.08) for reduced ICU length of stay and duration of mechanical ventilation. Overall mortality, hospital length of stay and infectious complications were unaffected. As noted earlier, the potential mechanisms underlying these actions are multiple. EPA/DHA are substrates for the production of IRMs which cannot be made if the parent compounds are not present. Examples of some of the functions of IRMs were summarized by Calder as, “Resolvin E1, resolvin D1 and protectin D1 all inhibit trans-endothelial migration of neutrophils, so preventing the infiltration of neutrophils into sites of inflammation; resolvin D1 inhibits IL-1β production and protectin D1 inhibits TNF-α and IL-1β production.” [46] Higher EPA/DHA levels reduce arachidonic acid (the omega-6 cousin of EPA) membrane levels [47] for the production of some pro-inflammatory oxylipins (certain prostaglandins and leukotrienes). Quite independently of the synthesis of these mediators, the presence of EPA/DHA in inflammatory cells blocks the activation of the key pro-inflammatory transcription factor, nuclear factor kappa B thus retarding the entire intracellular inflammatory cascade [48,49]. This effect is downstream from the action of these fatty acids on membrane G-protein coupled receptors GPR40 and GPR120 and nuclear peroxisome proliferator-activated receptors (reviewed in [50]). Finally, EPA/DHA insert into cell membrane phospholipids and disrupts lipid rafts so as to disassemble surface receptors thereby blocking incoming inflammatory signals [51]. All of these actions together result in a muted “cytokine storm” which, in alveolar macrophages and elsewhere, can result in death from COVID-19 [3]. 4.1. Limitations Given the pilot nature of this exploratory study, a number of limitations are acknowledged. Firstly, the sample size was small and further studies are needed to replicate this finding and to explore potential risk thresholds of the O3I. Secondly, the limited resources and resulting access to the full electronic medical record for more detailed chart review significantly reduced the amount of potentially relevant information on comorbidities and other demographic data besides age and sex (e.g., BMI). Although data on maximal interventions applied during hospitalization were available, the reasons why any given patient was administered a given treatment are not known and could obviously have been influenced by external factors (e.g., ventilator availability) or internal factors (e.g., a DNR order). Accordingly, such information was deemed to be of little utility in this pilot study. The population of patients in this study had an O3I that was typical of the US[39], which unfortunately means that levels were generally low. Future studies should endeavor to include patients with a wider range of O3I to examine these relationships more clearly. 4.2. Conclusions Given the profound public health concerns related to the current COVID-19 pandemic, modifiable risk factors for developing severe and critical complications are urgently needed. Despite the known mechanisms by which IRMs and omega-3 fatty acids support the active, endogenous resolution of inflammatory mechanisms, to our knowledge this is the first study that has explored the relationship between omega 3 tissue levels and the most severe COVID-19 outcome, death. Larger studies are urgently needed to confirm these findings. If an association is confirmed with a larger sample size, then this would lay the groundwork for testing the effects of increased oily fish intake and/or an inexpensive, safe, and widely available dietary supplement (DHA/EPA capsules) to optimize outcomes during this public health crisis. Author disclosure statements WSH holds an interest in OmegaQuant Analytics, LLC; and is a member of the Schiff Science and Innovation Advisory Board. The other authors have no conflicts of interest to disclose. Data availability statement The data that support the findings of this study are available from the corresponding author upon reasonable request. Funding statement This study was supported in part by Cedars-Sinai Medical Center (through the Cancer Clinical Trials Office), by the Fatty Acid Research Institute (for biostatistical support), and by a donation from Michael Myers (for blood analysis). CRediT authorship contribution statement Arash Asher: Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing - original draft. Nathan L. Tintle: Formal analysis, Writing - review & editing. Michael Myers: Conceptualization, Resources, Methodology, Writing - review & editing. Laura Lockshon: Project administration, Writing - review & editing. Heribert Bacareza: Project administration, Writing - review & editing. William S. Harris: Conceptualization, Methodology, Resources, Writing - original draft.
2021.03.07
學術分享 The effect of omega-3 fatty acid supplementation on clinical and biochemical parameters of critically ill patients with COVID-19: a randomized clinical trialPublished: 29 March 2021 The effect of omega-3 fatty acid supplementation on clinical and biochemical parameters of critically ill patients with COVID-19: a randomized clinical trial Saeid Doaei, Somayeh Gholami, Samira Rastgoo, Maryam Gholamalizadeh, Fatemeh Bourbour, Seyedeh Elaheh Bagheri, Forough Samipoor, Mohammad Esmail Akbari, Mahdi Shadnoush, Fereshteh Ghorat, Seyed Alireza Mosavi Jarrahi, Narjes Ashouri Mirsadeghi, Azadeh Hajipour, Parvin Joola, Alireza Moslem & Mark O. Goodarzi Journal of Translational Medicine volume 19, Article number: 128 (2021) Cite this article 11k Accesses 290 Altmetric Metricsdetails Abstract Background Omega-3 polyunsaturated fatty acids (n3-PUFAs) may exert beneficial effects on the immune system of patients with viral infections. This paper aimed to examine the effect of n3-PUFA supplementation on inflammatory and biochemical markers in critically ill patients with COVID-19. Methods A double-blind, randomized clinical trial study was conducted on 128 critically ill patients infected with COVID-19 who were randomly assigned to the intervention (fortified formula with n3-PUFA) (n = 42) and control (n = 86) groups. Data on 1 month survival rate, blood glucose, sodium (Na), potassium (K), blood urea nitrogen (BUN), creatinine (Cr), albumin, hematocrit (HCT), calcium (Ca), phosphorus (P), mean arterial pressure (MAP), O2 saturation (O2sat), arterial pH, partial pressure of oxygen (PO2), partial pressure of carbon dioxide (PCO2), bicarbonate (HCO3), base excess (Be), white blood cells (WBCs), Glasgow Coma Scale (GCS), hemoglobin (Hb), platelet (Plt), and the partial thromboplastin time (PTT) were collected at baseline and after 14 days of the intervention. Results The intervention group had significantly higher 1-month survival rate and higher levels of arterial pH, HCO3, and Be and lower levels of BUN, Cr, and K compared with the control group after intervention (all P < 0.05). There were no significant differences between blood glucose, Na, HCT, Ca, P, MAP, O2sat, PO2, PCO2, WBCs, GCS, Hb, Plt, PTT, and albumin between two groups. Conclusion Omega-3 supplementation improved the levels of several parameters of respiratory and renal function in critically ill patients with COVID-19. Further clinical studies are warranted. Trial registry Name of the registry: This study was registered in the Iranian Registry of Clinical Trials (IRCT); Trial registration number: IRCT20151226025699N3; Date of registration: 2020.5.20; URL of trial registry record: https://en.irct.ir/trial/48213 Introduction In recent years, coronavirus infections have been a significant source of morbidity and mortality around the world [1]. Novel coronavirus 2019 (nCoV-2019), now known as acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is responsible for the pandemic of coronavirus disease COVID-19 [2]. This infection usually causes a defined pattern of metabolic and clinical changes in affected patients [3]. Leukocytopenia, lymphopenia, and elevated C-reactive protein (CRP) can occur in the primary form of COVID-19. With disease progression, increasing levels of leukocytes, creatine kinase, and creatinine may also occur [4]. Host nutritional status has an important role in defense against viral infections [5]. Numerous studies have reported that malnourished humans are more susceptible to a wide variety of infections [6]. Indeed, proper nutrition can preserve the immune system and improve its function [7]. Nutritional deficiencies influence both immune response and viral pathogenic functions [5, 8]. Moreover, they may lead to oxidative stress in the host which can alter the genome of the virus, so that a normally benign or mildly pathogenic virus can convert to a highly virulent pathogen [6]. Omega-3 polyunsaturated fatty acids (n3-PUFAs) are important mediators of inflammation and acquired immune responses and can amplify anti-inflammatory responses [9]. Recent studies have been shown that n3-PUFAs including eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and α-linoleic acid (ALA) can increase the stability of the cell membrane, regulate immune function, block hyper inflammatory reactions, and reduce the incidence of systemic inflammatory response syndrome (SIRS), multiple organ dysfunction syndrome (MODS), and complications of infection [10]. Chen et al. reported a lower mortality rate in septic patients who received total parenteral nutrition containing 100 ml (ml) n3-PUFAs daily for 4 weeks. Also, the treatment group had a higher ratio of T helper to inducer lymphocytes and CD4 to CD8 lymphocytes in comparison with the control group during the first 7 days of follow-up [11]. Pluta et al. found that patients with chronic kidney disease, who daily received one capsule of omega 3 including 1000 mg n3-PUFAs containing 330 mg of EPA, 220 mg of DHA, and 100 mg of other acids such as alpha-linolenic acid (ALA) had lower urinary excretion of monocyte chemoattractant protein-1 (MCP-1) after 6 months of follow-up. However, white blood cell (WBC) count and serum levels of CRP and MCP-1 did not change significantly [12]. Soleimani et al. reported that patients with diabetic nephropathy, who received 1 g omega-3 acids daily had higher circulating nitric oxide (NO) after 12 weeks of follow-up with no change in serum concentrations of high sensitivity (hs)-CRP or total antioxidant capacity (TAC) [13]. Coghill et al. demonstrated that human immunodeficiency virus (HIV) and human herpesvirus-8 (HHV-8) co-infected patients, who received 3 gr of omega-3 fatty acids daily (each pill contained about 230 mg EPA and 150 mg DHA), had lower serum concentrations of the inflammatory cytokine interleukin-6 (IL-6) and higher CD8 + counts at 12 weeks [14]. Omar et al. in a recent study found that end-stage renal disease patients on chronic hemodialysis, who daily received two grams of omega-3 (containing 360 mg EPA and 240 mg DHA) had lower serum levels of IL-6 and CRP at 3 months [15]. On the other hand, Rice et al. conducted a randomized, double-blind, placebo-controlled, multicenter trial and reported that the n-3 supplementation did not improve the primary end point of ventilator-free days or other clinical outcomes in patients with acute lung injury and may be harmful. Patients receiving the n-3 supplement had fewer ventilator-free days, intensive care unit–free days, and nonpulmonary organ failure–free days [16] Given suggestive evidence of the beneficial effects of n3-PUFAs on the immune system and the contradictory results of recent studies concerning the effects of omega-3 fatty acids in patients with viral infections, we aimed to examine the effect of omega-3 supplementation on inflammatory and biochemical markers in critically ill patients with COVID-19. Methods Study design and population This study was a double-blind, randomized clinical trial study carried out from May to July 2020 in critically ill patients infected with COVID-19 in Razi Hospital, Rasht, Iran. The inclusion criteria were the age between 35 and 85 years, diagnosis of COVID-19 confirmed by a positive RT-PCR nasopharyngeal swab, as well as symptoms such as severe pneumonia, fever, fatigue, dry cough, respiratory distress, and indicated for enteral nutrition. One hundred thirty five patients were assessed for eligibility and 128 patients met the inclusion criteria. Sample size was calculated using α = 0.95, β = 20%, ratio of unexposed to exposed of 2:1, and power of 0.8. An unequal randomization ratio (2:1) was used because of a fixed and limited budget for this research project. Therefore, more participants were randomized to the cheaper arm in order to facilitate greater overall recruitment in the face of a possibly high drop-out rate. The exclusion criteria included history of cardiovascular and/or lung diseases (n = 4), and diagnosis of malignant tumors (n = 1) because of their effects on current medical treatment and diet, consumption of omega-3 fatty acids duing the prior 3 months before the study (n = 1), history of hypersensitivity reactions to fish or its products (n = 1), did not complete the study because of death (n = 14) or no indication for enteral feeding any more (n = 13). The final analysis was performed on 101 critically ill patients infected with COVID-19 who were assigned to the intervention (n = 28) and control (n = 73) groups. Interventions This study was done in form of a double-blind trial. Though no placebo was used, the patients were not aware of their feeding contents, and the patients and researchers were not aware of the arms of the study. Finally, the results were analyzed by a person outside of the treatment team. The allocation to the groups was done through web-based randomization using https://www.randomizer.org. Sealed non-transparent envelopes with randomized sequences were used to hide the allocation. All participants received high protein formula as 30 kcal/kg/d through enteral feeding. The intervention group received one capsule of 1000 mg omega-3 daily (Vita Pharmed, Switzerland) containing 400 mg EPAs and 200 mg DHAs for 14 days through adding the supplement to their enteral formula. Omega-3 fatty acids fortified formula was administered to the case group by a nurse, who was not a member of the research team, for 2 weeks after the first 24 h of hospitalization in ICU. The omega-3 capsules were pierced with a syringe, then its contents were squeezed out into a prepared enteral formula, with thorough mixing. The control group received nutritional support including the isocaloric-isovolemic formula using the same route, except for the intervention. Data collection After collecting the written consent forms, the required information was collected using a pre-determined checklist including the following sub-scales: Anthropometric and medical history Data on age, weight, height, previous illnesses, medications, blood pressure, serum lipids, random blood glucose, and respiratory status was collected using medical records. Dietary intake Data on nutritional intake including caloric intake, type of formula, and dietary supplements were assessed using documents recorded in ICU sheets and patient logs. Biochemical and pathological indices Arterial blood gas (ABG) parameters [i.e., O2 saturation, arterial pH, partial pressure of oxygen (PO2), partial pressure of carbon dioxide (PCO2), bicarbonate (HCO3), and base excess (Be)], kidney function parameters [i.e., blood urea nitrogen (BUN), creatinine (Cr), and urine volume], as well as blood glucose, mean arterial pressure, white cell blood count (including neutrophil, lymphocyte, monocyte), the Acute Physiology and Chronic Health Evaluation II (APACHE II), Glasgow Coma Scale (GCS), hemoglobin (Hb), platelet (Plt), the partial thromboplastin time (PTT), serum electrolytes [i.e. sodium (Na), potassium (K), calcium, phosphorus (P)], albumin, and hematocrit (Hct) were measured at baseline and after 14 days of the intervention. These measurements were routinely performed in the hospital using standard kits and the required data were gathered from the lab test section of the ICU sheets. Statistical analyses Quantitative data were presented as the mean ± standard deviation and qualitative data were presented as the percentage and number to describe the status of demographic, social, and anthropometric measurements of the participants. The Kolmogorov–Smirnov test was used to verify the normal distribution. Independent T-test and chi-square test were used to compare results between groups at baseline. The core research question was whether the difference between groups of interest changed from the basal values to the values after treatment. The general linear model repeated measure was used to identify the group-by-time interaction effect of omega-3 supplementation on inflammatory and biochemical markers, comparing the values in intervention and control groups. Confounding factors including age, sex, body mass index (BMI), dietary intake, smoking, presence of background diseases such as diabetes and hypertension, and medication and supplements were adjusted for. Statistical analyses were performed using the SPPS software (version 20). P values less than 0.05 were considered statistically significant. Results Patient characteristics A total of 135 eligible patients were included in this study and randomization was done 1:2. Of these, seven patients were excluded based on the exclusion criteria (Fig. 1). In addition, another seven patients in the treatment group and twenty controls were excluded from analysis after randomization, because they died during the intervention period. Finally, 101 patients were included in the analysis, of which 28 were assigned to the treatment group and 73 were assigned to the control group. All baseline data in Table 1 were normally distributed. The groups were not significantly different in demographic or clinical characteristics at baseline, except for the lymphocyte count, which was lower in the intervention group (11.59 vs 13.26, P = 0.01). Fig. 1 Study flowchart Full size image Table 1 Baseline demographic and clinical data of the study groups Full size table Effects of omega-3 supplementation on 1-month survival rate The intervention group had significantly higher 1-month survival rate compared with the control group (21% vs 3%, P = 0.003). About 21% (n = 6) of the participants in the intervention group and only about 3% (n = 2) of the participants in the control group survived at least for 1 month after the beginning of the study. Effects of omega-3 supplementation on kidney function As summarized in Table 2, levels of BUN (35.17 vs 43.19, F = 4.76, P = 0.03) and Cr (1.29 vs 1.68, F = 5.90, P = 0.02) were significantly lower and the amount of urine excreted (2101 vs 1877.02, F = 12.26, p = 0.01) was significantly higher in the intervention group compared with the control group. Table 2 Comparison of clinical and biochemical parameters between the intervention group and control group after the intervention Full size table Effects of omega-3 supplementation on arterial blood gas (ABG) parameters After 14 days, the levels of arterial pH (7.30 vs 7.26, F = 19.11, P = 0.01), HCO3 (22.00 vs 18.17, F = 10.83, P = 0.01), and Be (−4.97 vs −3.59, F = 23.01, P = 0.01) were significantly higher in the intervention group compared with the control group. However, there were no significant differences among PO2 and PCO2 between two groups (Table 2). Effects of omega-3 supplementation on the Glasgow coma scale (GCS) On admission to the study, the mean GCS was 8.37 in the intervention group and 7.90 in the control group (P > 0.05). As shown in Table 2, it was significantly lower after 14 days of the study in both groups (7.90 vs 7.49, F = 6.07, P = 0.05). No significant difference was found in APACHE II score between the groups (15.54 ± 1.73 vs 15.42 ± 1.92., P = 0.78). Effects of omega-3 supplementation on serum electrolytes As shown in Table 2, the level of K was significantly reduced in the intervention group compared to the control group (4.00 vs 4.14, F = 10.15, P = 0.01) after 14 days. No significant differences were found between the levels of serum electrolytes including Na, Ca, and P in between two groups after intervention. Effects of omega-3 supplementation on blood clotting function and cell blood count (CBC) The lymphocyte count increased in the omega-3 group compared to the control group, though this effect was marginally significant (11.59 vs 11.80, F = 4.08, P = 0.05). There were no significant differences in levels of PTT, hematocrit, neutrophil, monocyte, hemoglobin, and Plt between the two groups (Table 2). Effects of omega-3 supplementation on the other blood factors As shown in Table 2, no significant differences were observed in the other factors including blood glucose, albumin, MAP, and O2 sat between two groups after intervention. Discussion To our knowledge, this is the first randomized clinical trial assessing the effect of omega-3 fatty acid supplementation in ICU patients with COVID-19. We found that administration of omega-3 PUFA significantly improved arterial PH, HCO3, and Be. This trial also supports our hypothesis that omega-3 supplementation can improve the level of indicators of kidney function including BUN, Cr, K, and urine volume. The results have indicated that omega-3 supplementation may increase the lymphocyte count and GCS. However, these increases were not statistically significant. In our study, omega-3 supplementation had a positive effect on 1-month survival rate of the critically ill patients with COVID-19. Many severely or critically ill COVID-19 patients have been reported to develop severe metabolic and respiratory acidosis [17, 18], indicating possible microcirculation dysfunction [18]. This study identified that omega-3 supplementation improved arterial PH, HCO3, and Be, which may be related to the effect of omega-3 supplementation on microcirculatory function. Several studies [19,20,21] have reported that omega-3 supplementation improved endothelial function and microcirculation. Vasil'ev et al. reported that therapy with omega-3 PUFAs increased tissue hemoperfusion, capillary blood flow, and tissue blood flow and generally improved microcirculation. Trevor et al. studied the effects of DHA and EPA supplementation on vascular reactivity and microcirculation. They found that DHA significantly enhanced vasodilator mechanisms, attenuated constrictor responses, and improved endothelium reactivity and microcirculation [22] It has been reported that renal abnormalities occurred in the majority of patients with COVID-19 [18, 23,24,25], and microemboli in renal vessels as a consequence of the prothrombotic state results in kidney damage. Furthermore, hypertension induced by pro-inflammatory status, increasing IFN-γ, IL-6, and IL-17 expression and CD8 + T cells in the kidney, angiotensin II-induced hypertension, and the endothelial dysfunction caused by the innate immune response seems to be involved in the kidney injury [26]. Renal involvement in COVID-19 was reported to be associated with higher mortality [18, 23,24,25]. Hence, it is crucial to identify adjuvant and protective therapies that improve kidney function in patients with severe COVID-19. The present study found that the administration of omega-3 PUFAs significantly decreased BUN, Cr, and K and increased urine volume in ICU patients infected with COVID-19. These findings suggest that omega-3 supplementation may be protective against progression to renal impairment, consistent with observations from animal models that showed that omega-3 PUFA supplementation reduces the progression of renal disease [27,28,29,30,31]. Moreover, studies in human subjects suggested that a higher dietary intake of PUFAs may improve creatinine clearance [32] and also may have a role in maintaining healthy kidney function [33]. In contrast, some studies have reported that omega-3 treatment did not protect renal function. Higashihara et al. assessed the effects of omega-3 PUFAs on kidney function in 41 patients with stages two or three chronic kidney disease (CKD); omega-3 supplementation did not alter kidney function, assessed using 24-h urine creatinine clearance. Another study demonstrated that omega-3 PUFA pre-treatment did not protect against renal function deterioration or ischemia-induced renal inflammation; however, tubular transport was improved [30]. Previous studies that have evaluated omega-3 PUFAs in the treatment of kidney disease have yielded contradictory results, which may reflect differences in study duration, dosage of omega-3, route of administration, and type of omega-3 fatty acids. Omega-3 PUFAs can change the lipid composition and cell function of lymphocytes and affect cellular immune function [10, 34, 35]. There is no consensus regarding the efficacy of omega-3 PUFAs on lymphocyte count. A meta-analysis of randomized control trials found that the value of postoperative lymphocyte count increased in response to omega-3 PUFAs supplementation [10]. Consistent with this finding, the results of the present study identified a marginal increase in lymphocyte count after omega-3 PUFAs supplementation. The results of the current study identified a significant difference in 1-month survival rate between two groups. Supplementation with omega-3 fatty acids may have immune-modulating [36,37,38] and organ-protective effects [39, 40]. Previous studies have reported that higher plasma levels of omega-3 PUFAs are associated with survival [41,42,43]. Moreover, a recent systematic review found that omega-3 supplements can improve survival in critically ill patients [44]. However, another recent review article concluded that there is weak evidence for beneficial effects of omega-3 supplementation on ICU or hospitalized survival in critically ill patients [45]. Heller et al. have reported that the effects and effect sizes of omega-3 on clinical outcome is dependent on the disease [46]. Our study had some limitations. Although the sample size was calculated with an acceptable power for the study, the results need to be confirmed in larger studies. Moreover, only one dosage of omega-3 was used, which makes it difficult to discuss the dose–response efficacy of the supplement. It is possible that we may have seen more benefit with a higher dose. Another limitation of this study was the short duration of the study. Furthermore, prognostic biochemical markers in COVID-19 including the inflammatory cytokines C-reactive protein (CRP), interleukin-6, and interleukin-10, were not measured due to limited resources. Another limitation of this study was that there was no access to an omega-3 fatty acid enriched formula, and therefore we had to add it manually. Conclusion In conclusion, this randomized, double-blind, clinical trial has shown that omega-3 supplementation has promising effects on acidosis and renal function and possibly can improve clinical outcomes of patients infected with COVID-19. Further clinical studies with different dosages of n-3 PUFAs, larger sample sizes, and longer duration are warranted. Availability of data and materials All data will be made available upon request. Abbreviations n3-PUFAs: Omega-3 polyunsaturated fatty acids Na: Sodium K: Potassium BUN: Blood urea nitrogen Cr: Creatinine HCT: Hematocrit Ca: Calcium P: Phosphorus MAP: Mean arterial pressure O2 sat: O2 saturation PCO2 : Partial pressure of oxygen WBC: White blood cells

